Division of Hematology and Hematologic Malignancies, BIDMC, Boston, MA.
Division of Hematology and Hematologic Malignancies, BIDMC, Boston, MA, USA; Department of Medicine, Hematology Service, Memorial Sloan Kettering Cancer Center, New York, NY.
Haematologica. 2024 Jun 1;109(6):1849-1856. doi: 10.3324/haematol.2023.284192.
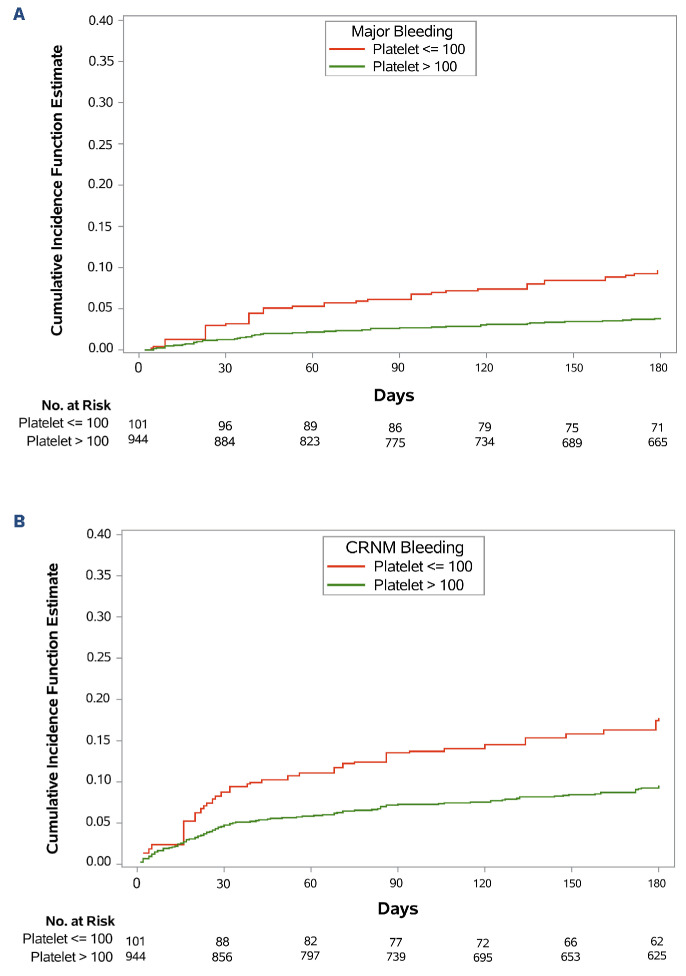
Thrombocytopenia occurs frequently in patients with cancer-associated thrombosis (CAT), however prospective evaluation of clinical outcomes following randomization to anticoagulants is limited. The HOKUSAI VTE Cancer study was a randomized, open-label, non-inferiority, phase III trial comparing dalteparin with edoxaban in CAT patients. This post hoc analysis of Hokusai VTE Cancer Study was performed to compare outcomes in patients with platelet count ≤100x109/L at one or more specified time points (baseline, 1-month, or 3-month) versus those without thrombocytopenia. Cumulative incidences at 180 days were calculated with death as a competing risk. The primary outcome was major bleeding; secondary outcomes were clinically relevant non-major bleeding (CRNMB), recurrent thrombosis, and survival. The analysis included 1,045 patients with primarily solid tumor malignancies (89%), median age 65 years, and 52% male. The thrombocytopenia group comprised 9.6% (N=101) of the cohort and relative to the non-thrombocytopenia cohort (N=944), experienced significantly higher major bleeding (9.0% vs. 4.0%, sub-distribution hazard ratio [SHR] =2.4; P=0.02) and CRNMB (17.9% vs. 9.6%, SHR=2.0; P=0.01). Thrombocytopenia did not impact recurrent venous thromboembolic event (VTE) (9.8% vs. 7.4%, SHR=1.3; P=0.37) nor overall mortality (21.8% vs. 26.0%, HR=0.9; P=0.48). Major bleeding was higher in patients with thrombocytopenia and gastrointestinal malignancies receiving edoxaban versus dalteparin (16.8% vs. 0; P<0.01) but similar for patients with other malignancies (P=0.30). In patients with hematologic malignances and thrombocytopenia major bleeding was higher for patients receiving dalteparin compared to edoxaban (19.0% vs. 0; P<0.01). Mild thrombocytopenia was associated with a doubling in risk of major hemorrhage in patients receiving anticoagulation for CAT. Bleeding risk for edoxaban and dalteparin varied in gastrointestinal and hematologic malignances in patients with thrombocytopenia (clinicaltrails gov. Identifier: NCT02073682).
癌症相关血栓形成(CAT)患者常发生血小板减少症,但针对抗凝治疗随机分组后临床结局的前瞻性评估有限。HOKUSAI VTE 癌症研究是一项随机、开放标签、非劣效性、III 期临床试验,比较了达肝素与依多沙班在 CAT 患者中的疗效。本 HOKUSAI VTE 癌症研究的事后分析旨在比较血小板计数在一个或多个特定时间点(基线、1 个月或 3 个月)≤100x109/L 的患者与无血小板减少症患者的结局。采用死亡作为竞争风险计算 180 天的累积发生率。主要结局为大出血;次要结局为临床相关非大出血(CRNMB)、复发性血栓形成和生存。该分析纳入了 1045 例主要为实体瘤恶性肿瘤(89%)的患者,中位年龄 65 岁,52%为男性。血小板减少症组占队列的 9.6%(N=101),与非血小板减少症组(N=944)相比,大出血(9.0%比 4.0%,亚分布风险比[SHR] =2.4;P=0.02)和 CRNMB(17.9%比 9.6%,SHR=2.0;P=0.01)发生率显著更高。血小板减少症并不影响复发性静脉血栓栓塞事件(VTE)(9.8%比 7.4%,SHR=1.3;P=0.37)或总体死亡率(21.8%比 26.0%,HR=0.9;P=0.48)。血小板减少症患者中,胃肠道恶性肿瘤患者接受依多沙班治疗的大出血发生率高于达肝素治疗者(16.8%比 0;P<0.01),但其他恶性肿瘤患者间无差异(P=0.30)。血液系统恶性肿瘤患者中,接受达肝素治疗者的大出血发生率高于接受依多沙班治疗者(19.0%比 0;P<0.01)。CAT 抗凝治疗患者中,轻度血小板减少症使大出血风险增加 1 倍。在血小板减少症患者中,依多沙班和达肝素在胃肠道和血液系统恶性肿瘤中的出血风险不同(临床试验.gov 标识符:NCT02073682)。