White Kyle C, Nasser Ahmad, Gatton Michelle L, Laupland Kevin B
Intensive Care Unit, Princess Alexandra Hospital, Woolloongabba, Queensland, Australia.
Faculty of Health, Queensland University of Technology (QUT), Brisbane, Queensland, Australia.
Crit Care Resusc. 2023 Jul 27;25(3):126-135. doi: 10.1016/j.ccrj.2023.06.002. eCollection 2023 Sep.
The overall objective of this scoping review is to assess the extent of the literature related to the fluid management of critically ill patients with acute kidney injury (AKI).
AKI is common in critically ill patients where fluid therapy is a mainstay of treatment. An association between fluid balance (FB) and adverse patient-centred outcomes in critically ill patients with AKI regardless of severity has been demonstrated. The evidence for the prospective intervention of FB and its impact on outcomes is unknown.
All studies investigating FB in patients with AKI admitted to an intensive care unit were included. Literature not related to FB in the critically ill patient with AKI population was excluded.
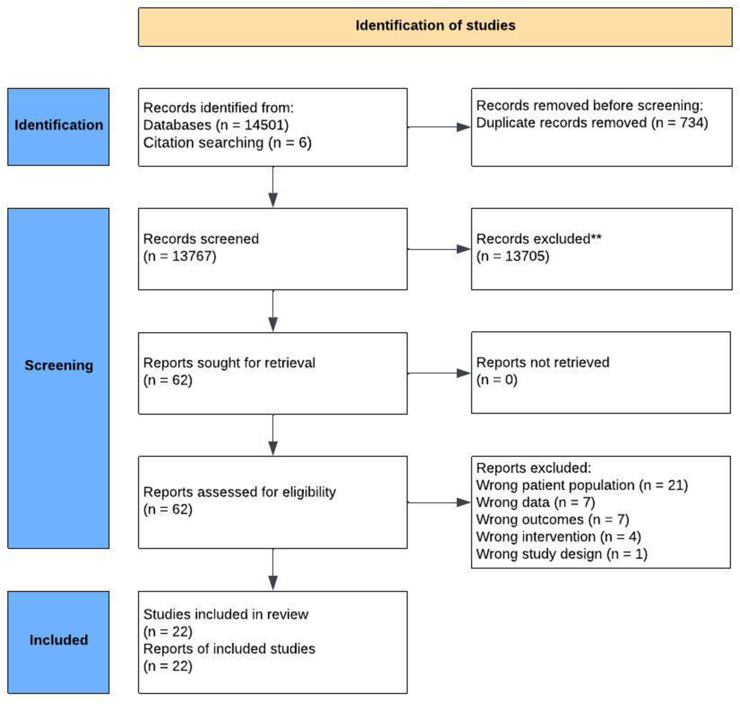
We searched MEDLINE, EMBASE, and CINAHL from January 1st, 2012, onwards. We included primary research studies, experimental and observational, recruiting adult participants admitted to an intensive care unit who had an AKI. We extracted data on study and patient characteristics, as well as FB, renal-based outcomes, and patient-centred outcomes. Two reviewers independently screened citations for eligible studies and performed data extraction.
Of the 13,767 studies reviewed, 22 met the inclusion criteria. Two studies examined manipulation of fluid input, 18 studies assessed enhancing fluid removal, and two studies applied a restrictive fluid protocol. Sixteen studies examined patients receiving renal replacement therapy, five studies included non-renal replacement therapy patients, and one study included both. Current evidence is broad with varied approaches to managing fluid input and fluid removal. The studies did not demonstrate a consensus approach for any aspect of the fluid management of critically ill patients. There was a limited application of a restrictive fluid protocol with no conclusions possible.
The current body of evidence for the management of FB in critically ill patients with AKI is limited in nature. The current quality of evidence is unable to guide current clinical practice. The key outcome of this review is to highlight areas for future research.
本综述的总体目标是评估与急性肾损伤(AKI)危重症患者液体管理相关的文献范围。
AKI在危重症患者中很常见,液体治疗是主要治疗手段。已证实,无论严重程度如何,AKI危重症患者的液体平衡(FB)与以患者为中心的不良结局之间存在关联。关于FB前瞻性干预及其对结局影响的证据尚不清楚。
纳入所有调查入住重症监护病房的AKI患者FB情况的研究。排除与AKI危重症患者群体中FB无关的文献。
我们检索了2012年1月1日起的MEDLINE、EMBASE和CINAHL数据库。我们纳入了招募入住重症监护病房且患有AKI的成年参与者的原发性研究,包括实验性和观察性研究。我们提取了关于研究和患者特征的数据,以及FB、基于肾脏的结局和以患者为中心的结局。两名评审员独立筛选符合条件的研究的引文并进行数据提取。
在审查的13767项研究中,22项符合纳入标准。两项研究探讨了液体输入的控制,18项研究评估了增加液体清除,两项研究应用了限制性液体方案。16项研究检查了接受肾脏替代治疗的患者,5项研究纳入了未接受肾脏替代治疗的患者,1项研究两者都包括。目前的证据广泛,在液体输入和液体清除管理方面有多种方法。这些研究在危重症患者液体管理的任何方面都未显示出一致的方法。限制性液体方案的应用有限,无法得出结论。
目前关于AKI危重症患者FB管理的证据在本质上是有限的。目前的证据质量无法指导当前的临床实践。本综述的关键结果是突出未来研究的领域。