Wu Wen-Qi, Zhang Yu-Qi, Xu Jie, Tang Zai-Xiang, Li Shi-Jia, Wei Xi-Ya, Li Ling, Wu He-Qing, Ma Xiao, Liu Ji-Sheng, Wu De-Pei, Wu Xiao-Jin
Department of Hematology, the First Affiliated Hospital of Soochow University, Suzhou, People's Republic of China.
National Clinical Research Center for Hematologic Diseases, Jiangsu Institute of Hematology, Suzhou, People's Republic of China.
Infect Drug Resist. 2023 Oct 25;16:6821-6831. doi: 10.2147/IDR.S424048. eCollection 2023.
The current study assesses which are the main risk factors, clinical outcome and prognosis following the colonization of CRE in patients that underwent allo-HSCT.
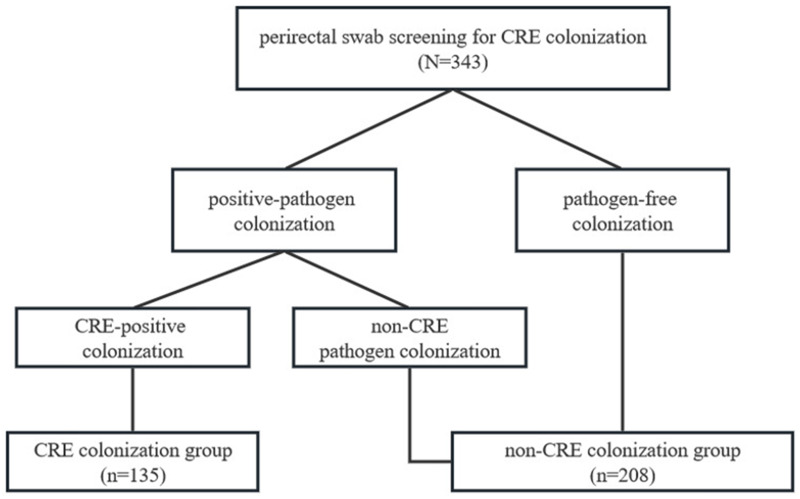
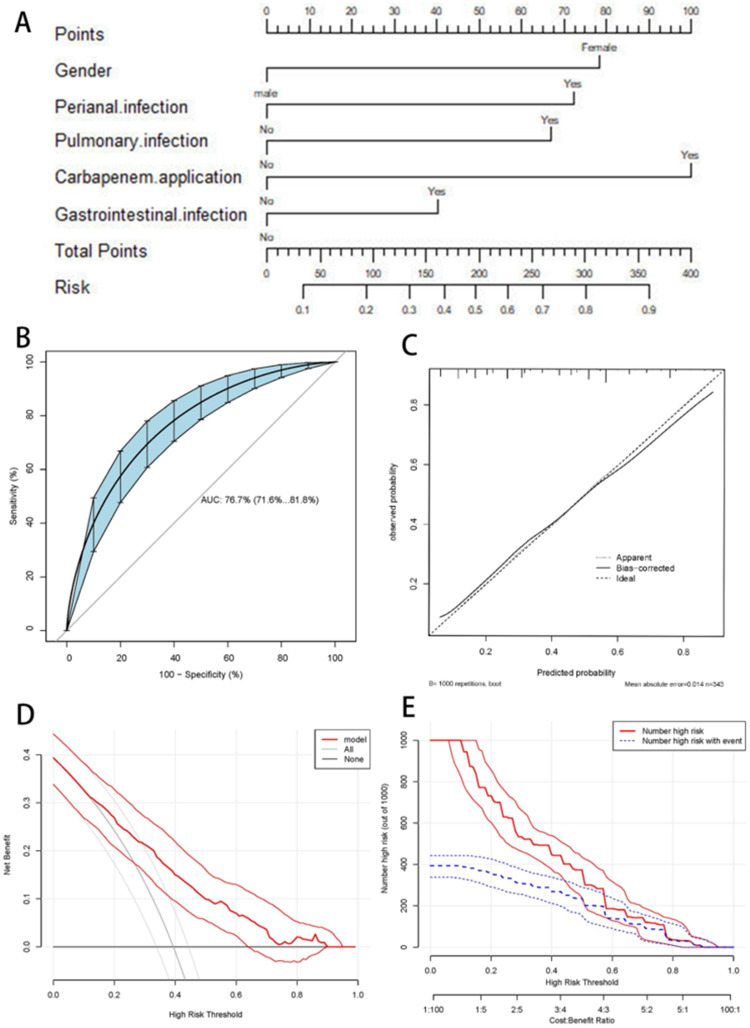
A total of 343 patients subjected to allo-HSCT in the period comprised between June 2021 and June 2022 were enrolled in this retrospective study. The CRE colonization was diagnosed by clinical history and routine microbial culture of perirectal swab. In this regard, a clinical prediction model was designed based on independent risk factors underlying the pre-transplantation CRE colonization using a backward stepwise logistic regression, followed by the evaluation of its discrimination and calibration efficacies, along with clinical usefulness. Furthermore, univariate and multivariate Cox regression analyses were then conducted to assess the risk factors for post-transplantation clinical outcomes.
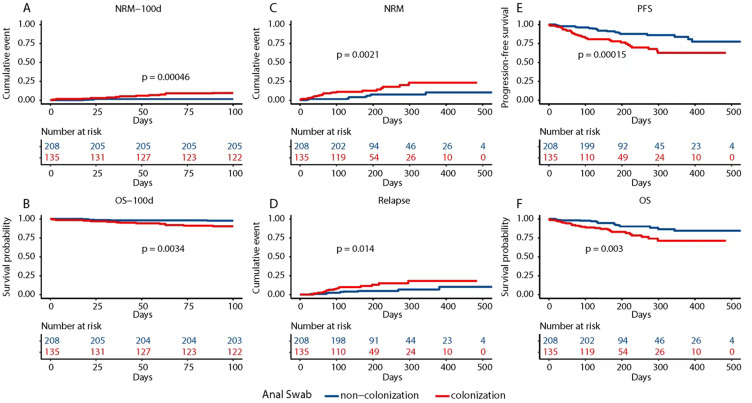
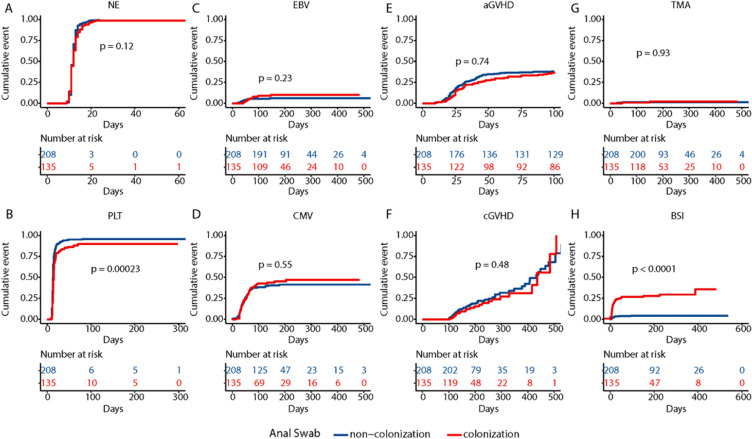
Out of 343 patients enrolled in this study, 135 (39.3%) reported CRE colonization. The independent risk factor variables for CRE colonization were incorporated into the nomogram to build a prediction model, which showed an area under the curve of 0.767 (95% CI: 0.716-0.818), and well-fitted calibration curves (χ2 = 1.737, P = 0.9788). The patients with CRE colonization reported a significantly lower platelet engraftment rate with a higher risk of post-transplantation BSI when compared with the non-CRE colonization group (P = 0.02 and P < 0.001; respectively). The non-relapse mortality (NRM) value was higher in the CRE patients (P < 0.05), consistently with a survival probability that was thus significantly lower for the same timeframe (P < 0.05).
A reliable clinical prediction model for pre-transplantation CRE colonization was developed that demonstrated that the CRE colonization negatively affects platelet engraftment and survival outcomes following allo-HSCT.
本研究评估接受异基因造血干细胞移植(allo-HSCT)的患者中耐碳青霉烯类肠杆菌(CRE)定植后的主要危险因素、临床结局和预后。
本回顾性研究纳入了2021年6月至2022年6月期间接受allo-HSCT的343例患者。通过临床病史和直肠拭子常规微生物培养诊断CRE定植。在此方面,基于移植前CRE定植的独立危险因素,采用向后逐步逻辑回归设计了一个临床预测模型,随后评估其区分度和校准效能以及临床实用性。此外,进行单因素和多因素Cox回归分析以评估移植后临床结局的危险因素。
在本研究纳入的343例患者中,135例(39.3%)报告有CRE定植。将CRE定植的独立危险因素变量纳入列线图以构建预测模型,该模型的曲线下面积为0.767(95%可信区间:0.716 - 0.818),校准曲线拟合良好(χ2 = 1.737,P = 0.9788)。与非CRE定植组相比,CRE定植患者的血小板植入率显著降低,移植后血流感染(BSI)风险更高(分别为P = 0.02和P < 0.001)。CRE患者的非复发死亡率(NRM)值更高(P < 0.05),同一时间段的生存概率也因此显著更低(P < 0.05)。
开发了一种可靠的移植前CRE定植临床预测模型,该模型表明CRE定植对allo-HSCT后的血小板植入和生存结局有负面影响。