Department of Clinical Oncology, Muhimbili University of Health and Allied Sciences, Dar Es Salaam, Tanzania.
Benjamin Mkapa Hospital, Dodoma, Tanzania.
J Med Case Rep. 2023 Nov 3;17(1):458. doi: 10.1186/s13256-023-04188-2.
Mycosis fungoides (MF) is the most common form of cutaneous T-cell lymphoma (CTCL). CTCL are an uncommon, heterogeneous group of non-Hodgkin lymphomas (NHLs) of T- and B-cell origin where the skin is the primary organ of involvement. It is characterized by malignant CD4 T-cells infiltrating the skin and other organs, leading to progressive skin and systemic involvement. Histopathologically, MF is characterized by atypical lymphocytes demonstrating epidermotropism without spongiosis. Spongiosis is the histological hallmark of intercellular epidermal edema, viewed as clear spaces within the epidermis, and is very common in benign inflammatory dermatoses. Very few studies have reported MF in sub-Saharan Africa (SSA). We are reporting a case of MF with a rare presentation of spongiosis treated successfully with a low dose total skin electron beam therapy (TSEBT) followed by maintenance therapy of low dose Methotrexate (MT) at the Ocean Road Cancer Institute (ORCI) in Tanzania. This is the first case of MF to be managed with low-dose TSEBT in Tanzania. The authors wish to create awareness of the disease among physicians and pathologists and expand on the data paucity in SSA.
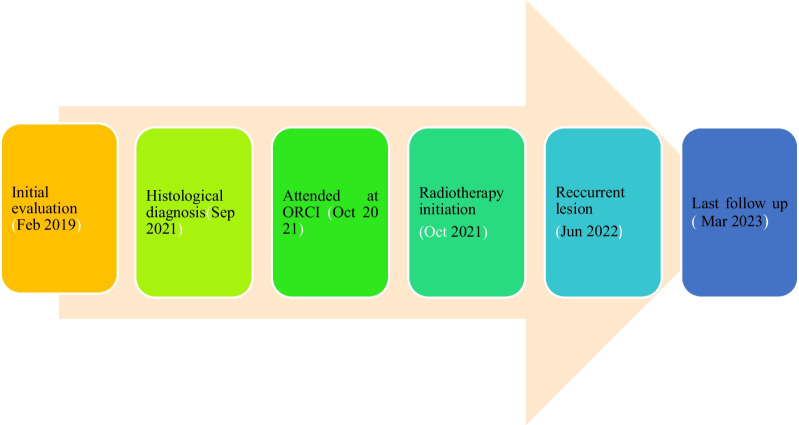
We are reporting a case of a 31-year-old male of African origin who self-referred to our oncology center with a 4-year history of skin rashes throughout the body, which was unresponsive to topical steroid treatment. The biopsy was taken, and the patient was diagnosed with MF CD 3 positive with spongiosis. The patient was treated with radiotherapy, whereby he received low dose total skin electron beam therapy (TSEBT) 12 Gy in 3 fractions at a daily dose of 4 Gy, followed by maintenance therapy of low dose Methotrexate and attained an excellent therapeutic response.
Spongiosis is an infrequent presentation of MF. Low-dose TSEBT provides reliable and rapid reduction of disease burden in patients with MF, which could be administered safely multiple times during a patient's disease with an acceptable toxicity profile. Lack of tendency to perform skin biopsies and cost constraints in assessing multiple immunophenotypic markers lead to missing the diagnosis. Diagnosis and treatment of MF in resource-limited countries is challenging.
蕈样真菌病(MF)是最常见的皮肤 T 细胞淋巴瘤(CTCL)形式。CTCL 是一组罕见的、异质性的非霍奇金淋巴瘤(NHL),起源于 T 细胞和 B 细胞,皮肤是主要受累器官。其特征是恶性 CD4 T 细胞浸润皮肤和其他器官,导致皮肤和全身进行性受累。组织病理学上,MF 的特点是具有表皮亲嗜性的非典型淋巴细胞,无海绵形成。海绵形成是细胞间表皮水肿的组织学标志,被视为表皮内的清晰空间,在良性炎症性皮肤病中非常常见。在撒哈拉以南非洲(SSA),很少有研究报告 MF。我们报告了一例罕见海绵形成的 MF 病例,采用低剂量全身电子束治疗(TSEBT)成功治疗,随后在坦桑尼亚的海洋路癌症研究所(ORCI)接受低剂量甲氨蝶呤(MT)维持治疗。这是坦桑尼亚首例采用低剂量 TSEBT 治疗的 MF 病例。作者希望在医生和病理学家中提高对该病的认识,并扩大 SSA 中数据的缺乏。
我们报告了一例 31 岁的非洲裔男性病例,他因全身皮疹 4 年,对局部类固醇治疗无反应,自行到我们的肿瘤中心就诊。进行了活检,患者被诊断为 MF CD3 阳性伴海绵形成。患者接受了放射治疗,接受了低剂量全身电子束治疗(TSEBT),共 3 次,每次 12 Gy,每天剂量 4 Gy,随后接受低剂量甲氨蝶呤维持治疗,获得了极好的治疗反应。
海绵形成是 MF 的一种不常见表现。低剂量 TSEBT 可可靠且快速地降低 MF 患者的疾病负担,可在患者疾病期间多次安全给予,具有可接受的毒性特征。由于缺乏进行皮肤活检的倾向和评估多种免疫表型标志物的费用限制,导致漏诊。资源有限国家的 MF 诊断和治疗具有挑战性。