Inflammatory Bowel Disease Center, University of Chicago Medicine, Chicago, IL, USA.
Takeda Pharmaceuticals USA, Inc, Lexington, MA, USA.
Inflamm Bowel Dis. 2024 Oct 3;30(10):1776-1787. doi: 10.1093/ibd/izad245.
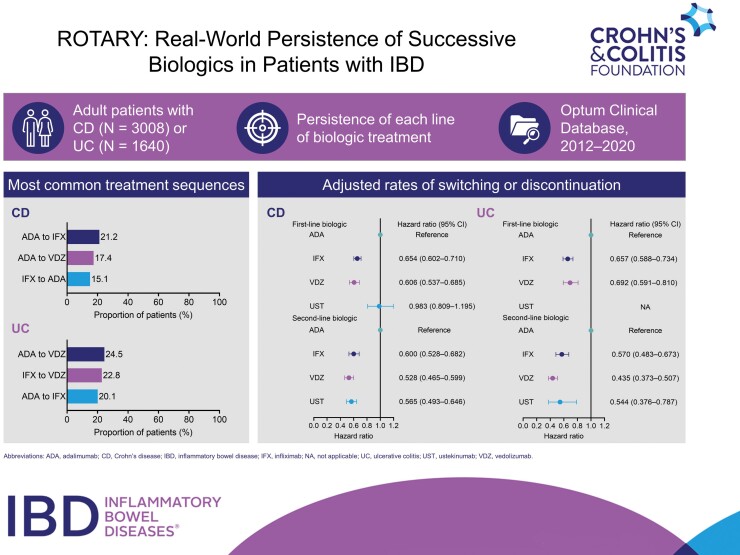
Patients with inflammatory bowel disease (IBD) may receive multiple successive biologic treatments in clinical practice; however, data are limited on the comparative effectiveness of biologics and the impact of treatment sequence on outcomes.
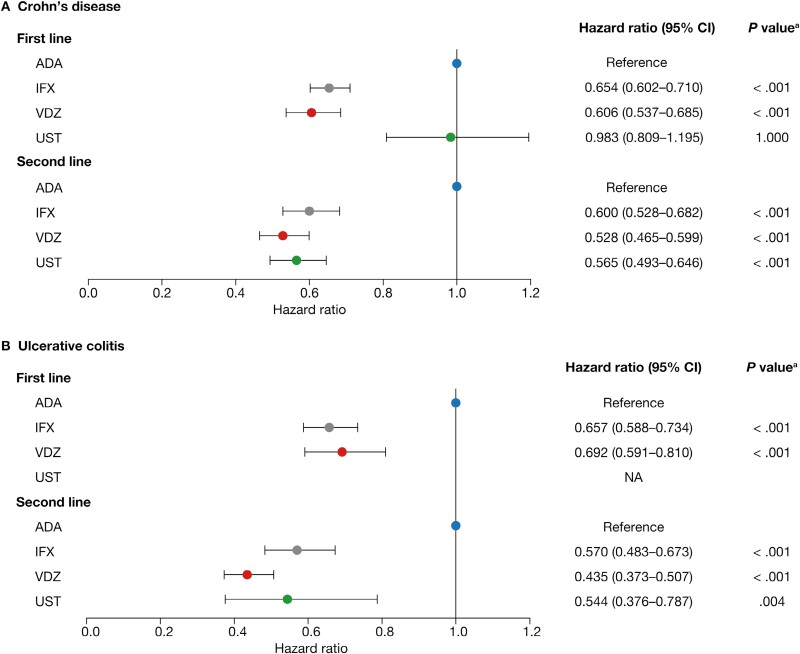
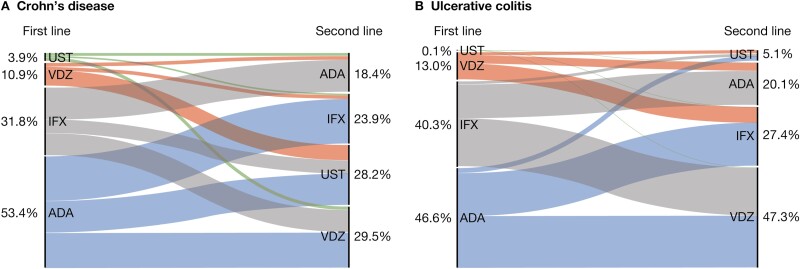
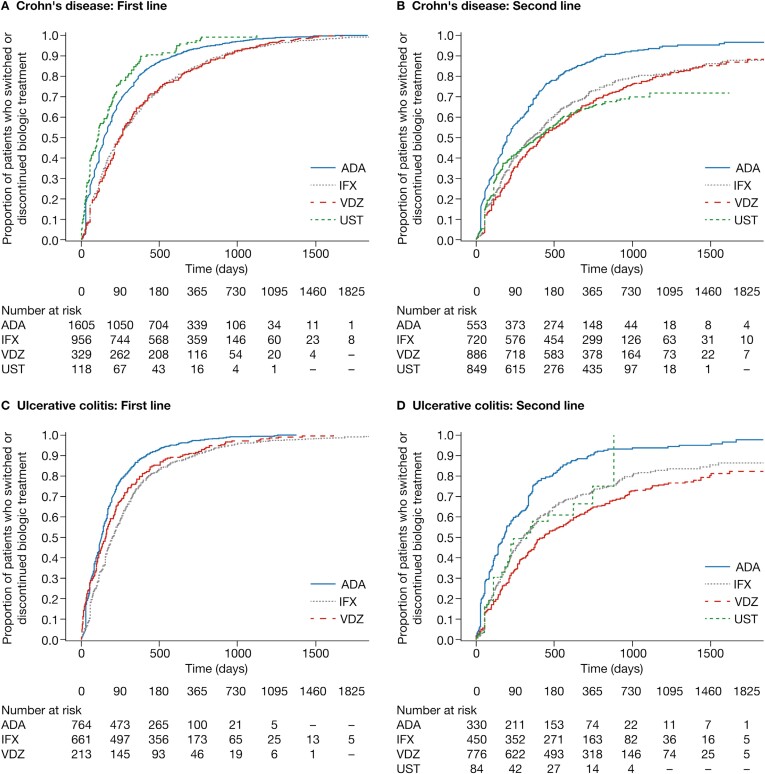
The ROTARY (Real wOrld ouTcomes Across tReatment sequences in inflammatorY bowel disease patients) study was a retrospective, observational cohort study conducted using data from the Optum Clinical Database between January 1, 2012, and February 29, 2020. Adult patients with Crohn's disease (CD) or ulcerative colitis (UC) who received 2 biologics successively were included. Biologic treatment sequences were analyzed descriptively. Cox proportional hazards models, adjusted for baseline demographics and clinical characteristics, were used to estimate the hazard ratio of switching or discontinuation for each first- and second-line biologic compared with first- and second-line adalimumab, respectively.
In total, 4648 patients with IBD (CD, n = 3008; UC, n = 1640) were identified. Most patients received tumor necrosis factor α antagonist (anti-TNFα) treatment followed by another anti-TNFα treatment or vedolizumab. Vedolizumab and infliximab had 39.4% and 34.6% lower rates of switching or discontinuation than adalimumab, respectively, as first-line biologics in patients with CD and 30.8% and 34.3% lower rates as first-line biologics in patients with UC, respectively. Vedolizumab, infliximab, and ustekinumab had 47.2%, 40.0%, and 43.5% lower rates of switching or discontinuation than adalimumab, respectively, as second-line biologics in CD and 56.5%, 43.0%, and 45.6% lower rates as second-line biologics in patients with UC, respectively.
Although anti-TNFα treatments were most commonly prescribed, the adjusted rates of discontinuation for adalimumab as both a first- and second-line biologic were higher than for vedolizumab, infliximab, or ustekinumab.
在临床实践中,患有炎症性肠病(IBD)的患者可能会接受多次连续的生物治疗;然而,关于生物制剂的比较效果以及治疗顺序对结果的影响的数据有限。
ROTARY(治疗序列对炎症性肠病患者的真实世界结果)研究是一项回顾性观察队列研究,使用了 2012 年 1 月 1 日至 2020 年 2 月 29 日期间 Optum 临床数据库中的数据。纳入接受 2 种生物制剂连续治疗的成年克罗恩病(CD)或溃疡性结肠炎(UC)患者。对生物治疗顺序进行描述性分析。使用 Cox 比例风险模型,根据基线人口统计学和临床特征进行调整,分别估计每种一线和二线生物制剂与一线和二线阿达木单抗相比转换或停药的风险比。
共纳入 4648 例 IBD 患者(CD,n=3008;UC,n=1640)。大多数患者接受肿瘤坏死因子-α拮抗剂(抗-TNFα)治疗,随后接受另一种抗-TNFα治疗或 vedolizumab。在 CD 患者中,vedolizumab 和 infliximab 作为一线生物制剂的转换或停药率分别比阿达木单抗低 39.4%和 34.6%,在 UC 患者中,vedolizumab 和 infliximab 作为一线生物制剂的转换或停药率分别比阿达木单抗低 30.8%和 34.3%。在 CD 患者中,vedolizumab、infliximab 和 ustekinumab 作为二线生物制剂的转换或停药率分别比阿达木单抗低 47.2%、40.0%和 43.5%,在 UC 患者中,vedolizumab、infliximab 和 ustekinumab 作为二线生物制剂的转换或停药率分别比阿达木单抗低 56.5%、43.0%和 45.6%。
尽管抗-TNFα治疗最常被开处方,但阿达木单抗作为一线和二线生物制剂的停药率调整后均高于 vedolizumab、infliximab 或 ustekinumab。