Inflammatory Bowel Disease Center, University of Chicago Medicine, Chicago, IL, USA.
Takeda Pharmaceuticals U.S.A., Inc., Lexington, MA, USA.
BMC Gastroenterol. 2024 Sep 17;24(1):314. doi: 10.1186/s12876-024-03378-6.
Patients with inflammatory bowel disease (IBD) are at risk of developing dysplasia and, subsequently, colorectal cancer (CRC) owing to chronic inflammation. Patients may also experience other severe disease complications, such as hospitalization and surgery. Several biologics are available for the treatment of patients with IBD and some patients require multiple lines of treatment owing to loss of response or tolerability to their prescribed biologic. Previous studies suggest that the choice of initial biologic treatment may impact the outcomes of later treatment lines. In this study, we assessed adverse clinical outcomes in patients with Crohn's disease (CD) or ulcerative colitis (UC) who received different biologic treatment sequences.
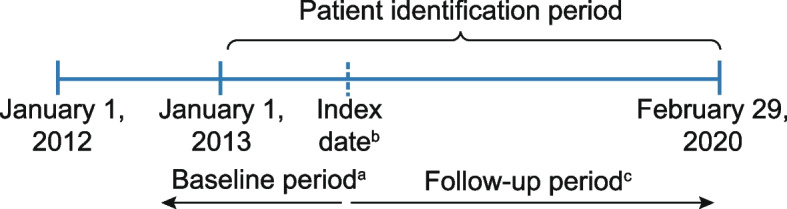
ROTARY part B was a retrospective cohort study using the Optum® Clinical Database that evaluated the incidences of IBD-related hospitalization, IBD-related surgery, dysplasia, CRC, and infections in patients with CD or UC who received two biologics successively. First-line biologics included adalimumab, infliximab, ustekinumab (CD only), and vedolizumab; second-line biologics included infliximab and adalimumab.
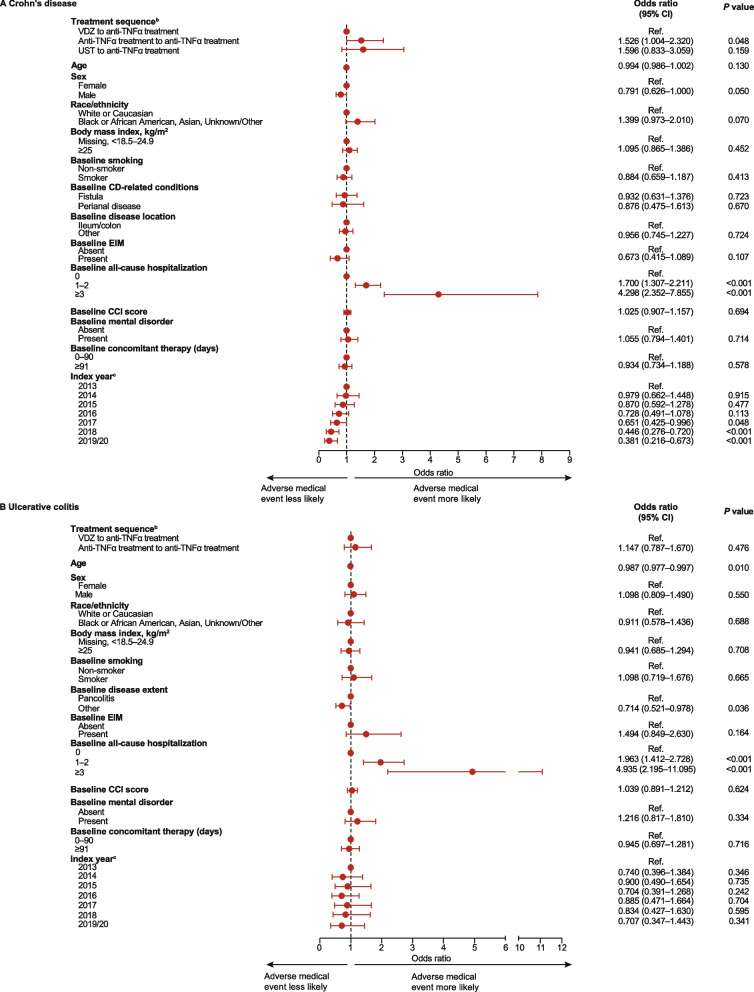
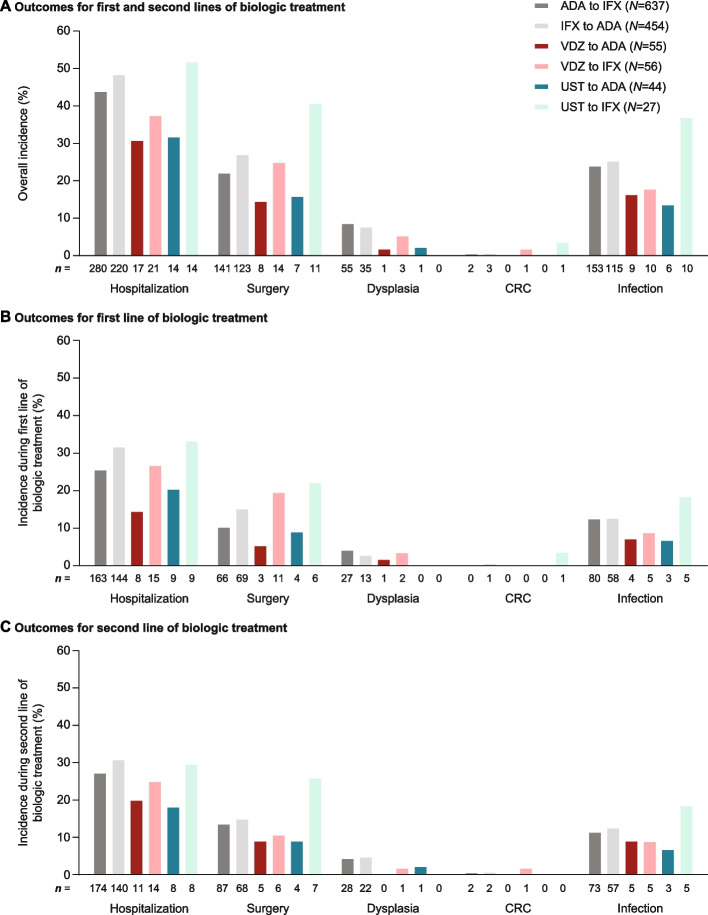
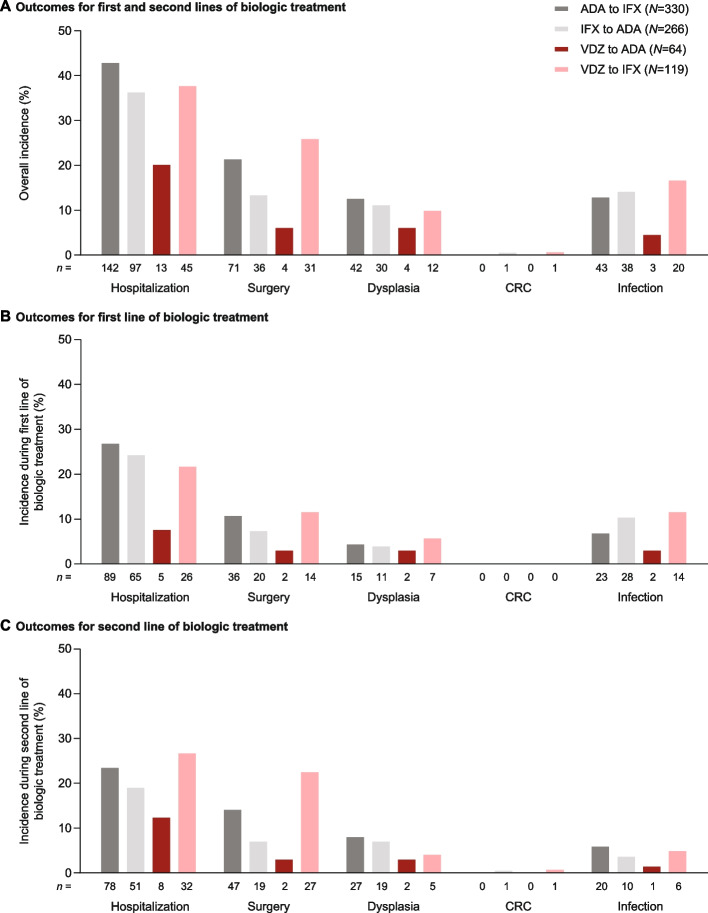
In patients with CD, the treatment sequence of ustekinumab to infliximab was associated with the highest overall incidences of hospitalization (51.9%), surgery (40.7%), CRC (3.7%), and infection (37.0%). Vedolizumab followed by an anti-tumor necrosis factor alpha (anti-TNFα) treatment was associated with a significantly lower risk of experiencing an adverse medical event (hospitalization, surgery, or infection) than two successive anti-TNFα treatments (odds ratio, 1.526; 95% confidence interval, 1.004-2.320; P < 0.05). In patients with UC, the treatment sequence of vedolizumab to adalimumab resulted in the lowest overall incidence of adverse outcomes (20.3%, 6.3%, 0.0%, 6.3%, and 4.7% for hospitalization, surgery, CRC, dysplasia, and infection, respectively).
We describe differences in adverse clinical outcomes associated with sequencing of biologics in patients with CD or UC and demonstrate favorable results in patients who received vedolizumab as a first-line biologic. These results provide potential guidance to clinicians choosing sequences of biologic treatments in patients with IBD.
由于慢性炎症,炎症性肠病(IBD)患者存在发生异型增生和结直肠癌(CRC)的风险。患者还可能经历其他严重疾病并发症,如住院和手术。有几种生物制剂可用于治疗 IBD 患者,由于对规定的生物制剂失去反应或耐受性,一些患者需要进行多线治疗。先前的研究表明,初始生物制剂治疗的选择可能会影响后续治疗线的结果。在这项研究中,我们评估了接受不同生物制剂治疗方案的克罗恩病(CD)或溃疡性结肠炎(UC)患者的不良临床结局。
ROTARY 研究 B 部分是一项回顾性队列研究,使用 Optum®临床数据库评估了连续接受两种生物制剂治疗的 CD 或 UC 患者中与 IBD 相关的住院、与 IBD 相关的手术、异型增生、CRC 和感染的发生率。一线生物制剂包括阿达木单抗、英夫利昔单抗、乌司奴单抗(仅用于 CD)和维得利珠单抗;二线生物制剂包括英夫利昔单抗和阿达木单抗。
在 CD 患者中,乌司奴单抗序贯英夫利昔单抗的治疗方案与最高的总住院率(51.9%)、手术率(40.7%)、CRC 发生率(3.7%)和感染率(37.0%)相关。维得利珠单抗序贯抗肿瘤坏死因子-α(抗-TNFα)治疗与连续两种抗-TNFα治疗相比,发生不良医疗事件(住院、手术或感染)的风险显著降低(比值比,1.526;95%置信区间,1.004-2.320;P<0.05)。在 UC 患者中,维得利珠单抗序贯阿达木单抗的治疗方案导致不良结局的总发生率最低(住院、手术、CRC、异型增生和感染的发生率分别为 20.3%、6.3%、0.0%、6.3%和 4.7%)。
我们描述了 CD 或 UC 患者中生物制剂序贯治疗相关的不良临床结局差异,并在接受维得利珠单抗作为一线生物制剂的患者中观察到了有利结果。这些结果为临床医生在选择 IBD 患者的生物制剂治疗方案时提供了潜在的指导。