Renal Division, Department of Medicine, Brigham and Women's Hospital, Boston, Massachusetts.
Harvard Medical School, Boston, Massachusetts.
JAMA Cardiol. 2024 Feb 1;9(2):144-152. doi: 10.1001/jamacardio.2023.4664.
An initial decline in estimated glomerular filtration rate (eGFR) is expected after initiating a sodium-glucose cotransporter-2 inhibitor (SGLT2i) and has been observed across patients with diabetes, chronic kidney disease, and heart failure.
To examine the implications of initial changes in eGFR among patients with heart failure with mildly reduced ejection fraction (HFmrEF) or preserved ejection fraction (HFpEF) enrolled in the Dapagliflozin Evaluation to Improve the Lives of Patients With Preserved Ejection Fraction Heart Failure (DELIVER) trial.
DESIGN, SETTING, AND PARTICIPANTS: This was a prespecified analysis of the results of the DELIVER randomized clinical trial, which was an international multicenter study of patients with EF greater than 40% and eGFR greater than or equal to 25. The DELIVER trial took place from August 2018 to March 2022. Data for the current prespecified study were analyzed from February to October 2023.
Dapagliflozin, 10 mg per day, or placebo.
In this prespecified analysis, the frequency of an initial eGFR decline (baseline to month 1) was compared between dapagliflozin and placebo. Cox models adjusted for baseline eGFR and established prognostic factors were fit to estimate the association of an initial eGFR decline with cardiovascular (cardiovascular death or heart failure event) and kidney (≥50% eGFR decline, eGFR<15 or dialysis, death from kidney causes) outcomes, landmarked at month 1, stratified by diabetes.
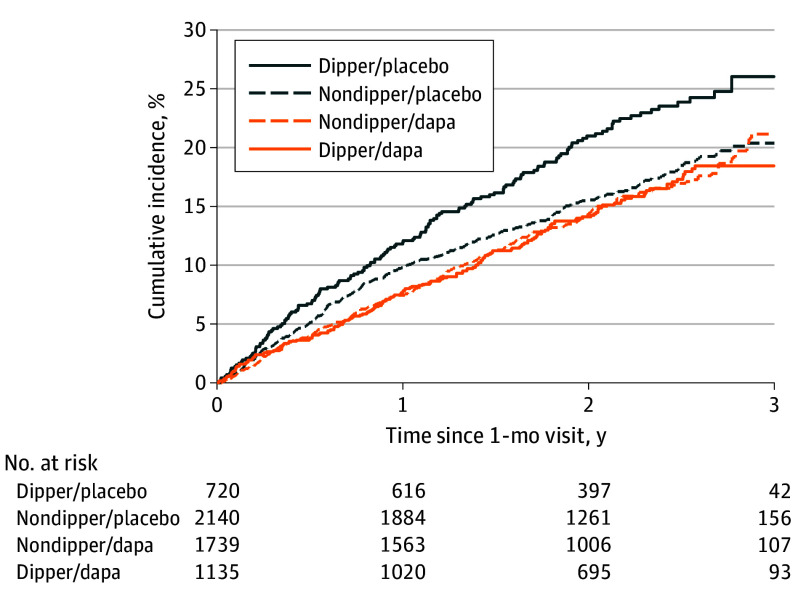
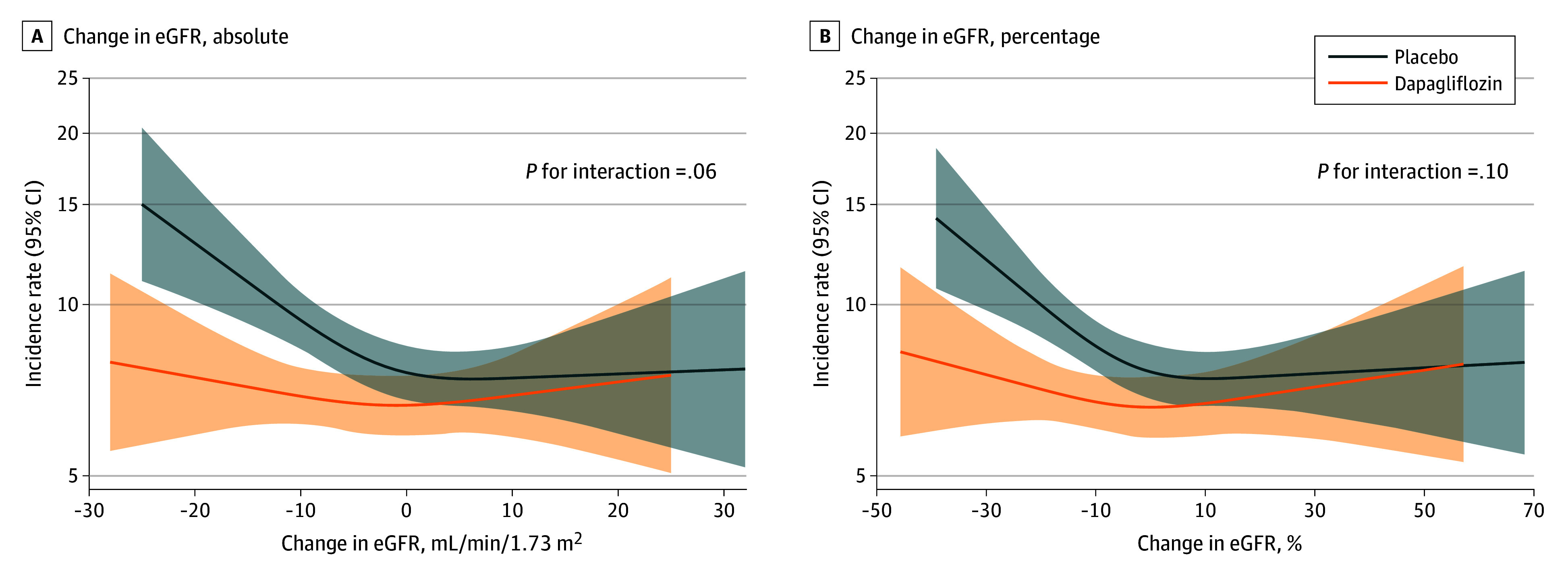
Study data from 5788 participants (mean [SD] age, 72 [10] years; 3253 male [56%]) were analyzed. The median (IQR) change in eGFR level from baseline to month 1 was -1 (-6 to 5) with placebo and -4 (-9 to 1) with dapagliflozin (difference, -3; P < .001). A higher proportion of patients assigned to dapagliflozin developed an initial eGFR decline greater than 10% vs placebo (1144 of 2892 [40%] vs 737 of 2896 [25%]; odds ratio, 1.9; 95% CI, 1.7-2.1; P difference <.001). An initial eGFR decline of greater than 10% (vs ≤10%) was associated with a higher risk of the primary cardiovascular outcome among those randomized to placebo (adjusted hazard ratio [aHR], 1.33; 95% CI, 1.10-1.62) but not among those randomized to dapagliflozin (aHR, 0.90; 95% CI, 0.74-1.09; P for interaction = .01). Similar associations were observed when alternative thresholds of initial eGFR decline were considered and when analyzed as a continuous measure. An initial eGFR decline of greater than 10% was not associated with adverse subsequent kidney composite outcomes in dapagliflozin-treated patients (aHR, 0.94; 95% CI, 0.49-1.82).
Among patients with HFmrEF or HFpEF treated with dapagliflozin, an initial eGFR decline was frequent but not associated with subsequent risk of cardiovascular or kidney events. These data reinforce clinical guidance that SGLT2is should not be interrupted or discontinued in response to an initial eGFR decline.
ClinicalTrials.gov Identifier: NCT03619213.
在开始使用钠-葡萄糖共转运蛋白 2 抑制剂 (SGLT2i) 后,预计估计肾小球滤过率 (eGFR) 会最初下降,这种情况在糖尿病、慢性肾脏病和心力衰竭患者中均有观察到。
检查心力衰竭伴轻度射血分数降低 (HFmrEF) 或射血分数保留 (HFpEF) 的患者在 Dapagliflozin Evaluation to Improve the Lives of Patients With Preserved Ejection Fraction Heart Failure (DELIVER) 试验中接受达格列净治疗后的 eGFR 最初变化的影响。
设计、地点和参与者:这是 DELIVER 随机临床试验结果的预先指定分析,该研究是一项国际多中心研究,纳入了 EF 大于 40% 和 eGFR 大于或等于 25 的患者。DELIVER 试验于 2018 年 8 月至 2022 年 3 月进行。目前预先指定的研究的数据分析于 2023 年 2 月至 10 月进行。
达格列净,每天 10mg,或安慰剂。
在这项预先指定的分析中,比较了达格列净和安慰剂之间最初 eGFR 下降(基线至第 1 个月)的频率。调整了基线 eGFR 和既定预后因素的 Cox 模型被用来估计最初 eGFR 下降与心血管(心血管死亡或心力衰竭事件)和肾脏(≥50% eGFR 下降、eGFR<15 或透析、肾脏原因导致的死亡)结局的关联,以第 1 个月为时间点,按糖尿病分层。
对 5788 名参与者(平均[SD]年龄 72[10]岁;男性 3253 名[56%])的数据进行了分析。与安慰剂相比,达格列净治疗组从基线到第 1 个月 eGFR 水平的中位数(IQR)变化为-1(-6 至 5),而安慰剂组为-4(-9 至 1)(差异,-3;P<0.001)。与安慰剂相比,更多接受达格列净治疗的患者出现 eGFR 下降大于 10%(达格列净组 2892 名患者中的 1144 名[40%] vs 安慰剂组 2896 名患者中的 737 名[25%];比值比,1.9;95%CI,1.7-2.1;P 差异<.001)。与安慰剂相比,eGFR 下降大于 10%(与≤10%相比)与主要心血管结局风险增加相关(调整后的危险比[aHR],1.33;95%CI,1.10-1.62),但与接受达格列净治疗的患者无相关性(aHR,0.90;95%CI,0.74-1.09;P 交互作用=.01)。当考虑替代初始 eGFR 下降阈值和作为连续测量时,也观察到类似的关联。在接受达格列净治疗的患者中,eGFR 下降大于 10% 与随后的肾脏复合结局不良无关(aHR,0.94;95%CI,0.49-1.82)。
在接受达格列净治疗的 HFmrEF 或 HFpEF 患者中,最初的 eGFR 下降很常见,但与随后的心血管或肾脏事件风险无关。这些数据强化了临床指导,即不应因初始 eGFR 下降而中断或停止 SGLT2i 的使用。
ClinicalTrials.gov 标识符:NCT03619213。