Mayer Kristine E, Gaa Jochen, Wasserer Sophia, Biedermann Tilo, Persa Oana-Diana
Clinic and Policlinic for Dermatology and Allergology, Technical University Munich, 80802 Munich, Germany.
Institute for Diagnostic and Interventional Radiology, Technical University Munich, 81675 Munich, Germany.
Cancers (Basel). 2023 Nov 2;15(21):5265. doi: 10.3390/cancers15215265.
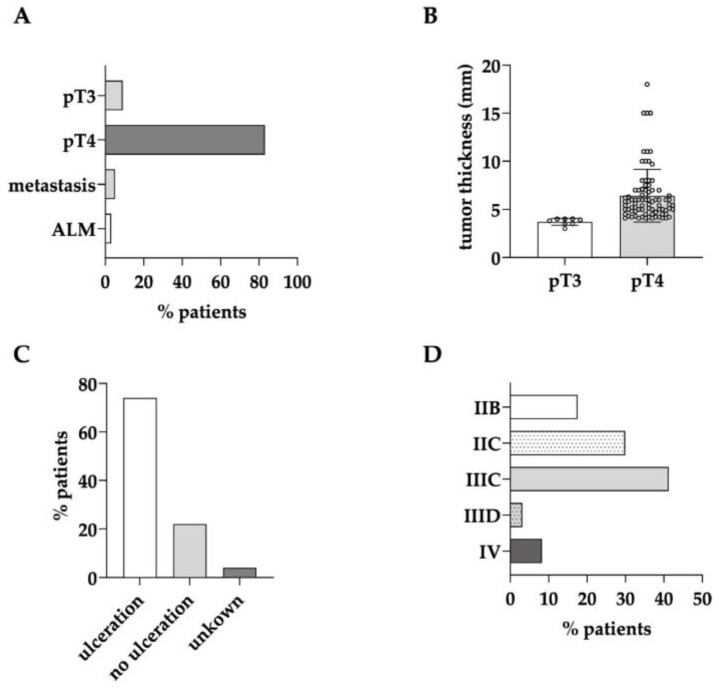
Melanoma staging at diagnosis predominantly depends on the tumor thickness. Sentinel lymph node biopsy (SLNB) is a common tool for primary staging. However, for tumors of >4 mm with ulceration, 3D whole-body imaging and, in particular, Fluor-18-Deoxyglucose positron emission tomography combined with computed tomography (F-FDG-PET/CT), is recommended beforehand. This study aimed to investigate the real-world data of whole-body imaging for initial melanoma staging and its impact on the subsequent diagnostic and therapeutic procedures.
In this retrospective single-center study, 94 patients receiving F-FDG-PET/CT and six patients with whole-body computed tomography (CT) scans were included. The clinical characteristics, imaging results, and histologic parameters of the primary tumors and metastases were analyzed.
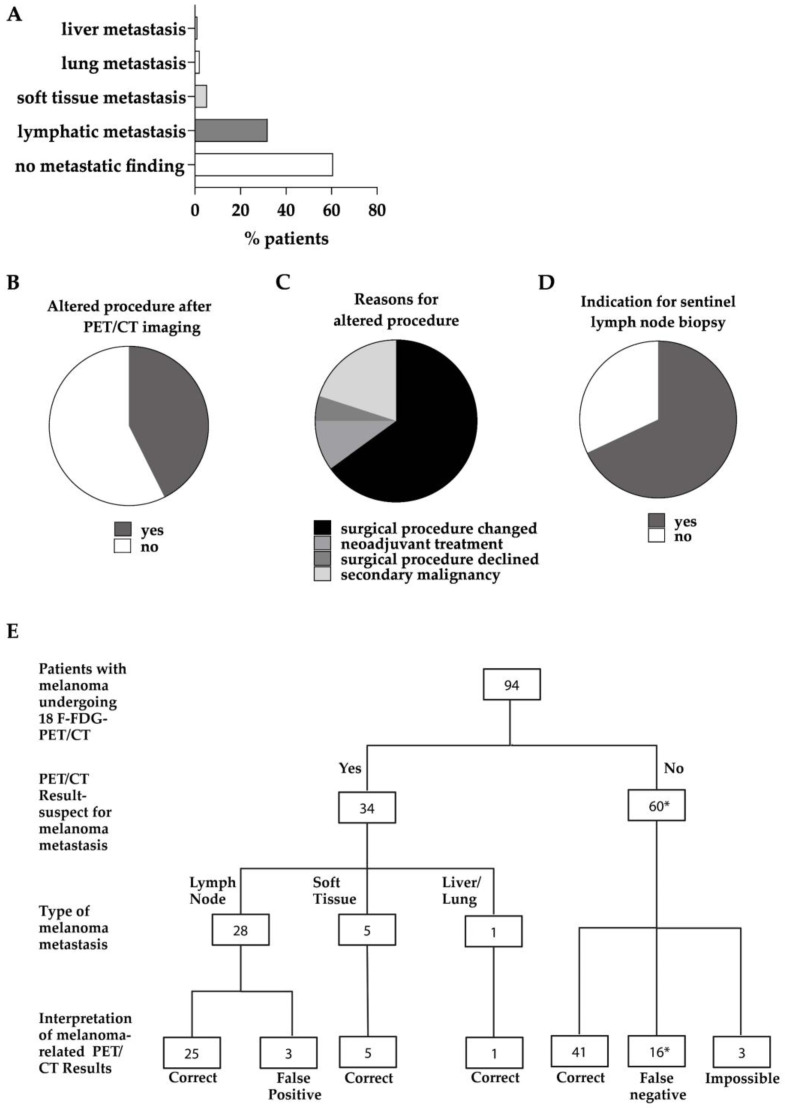
Besides the patients with primary tumors characterized as pT4b (63%), the patients with pT4a tumors and pT3 tumors close to 4 mm in tumor thickness also received initial whole-body imaging. In 42.6% of the patients undergoing F-FDG-PET/CT, the imaging results led to a change in the diagnostic or therapeutic procedure following on from this. In 29% of cases, sentinel lymph node biopsy was no longer necessary. The sensitivity and specificity of F-FDG-PET/CT were 66.0% and 93.0%, respectively.
Whole-body imaging as a primary diagnostic tool is highly valuable and influences the subsequent diagnostic and therapeutic procedures in a considerable number of patients with a relatively high tumor thickness. It can help avoid the costs and invasiveness of redundant SLNB and simultaneously hasten the staging of patients at the time of diagnosis.
黑色素瘤诊断时的分期主要取决于肿瘤厚度。前哨淋巴结活检(SLNB)是主要分期的常用手段。然而,对于厚度>4mm且伴有溃疡的肿瘤,建议预先进行三维全身成像,尤其是氟-18-脱氧葡萄糖正电子发射断层扫描联合计算机断层扫描(F-FDG-PET/CT)。本研究旨在调查全身成像用于黑色素瘤初始分期的真实世界数据及其对后续诊断和治疗程序的影响。
在这项回顾性单中心研究中,纳入了94例接受F-FDG-PET/CT检查的患者和6例接受全身计算机断层扫描(CT)的患者。分析了原发性肿瘤和转移灶的临床特征、影像学结果和组织学参数。
除原发性肿瘤特征为pT4b的患者(63%)外,肿瘤厚度接近4mm的pT4a肿瘤和pT3肿瘤患者也接受了初始全身成像。在接受F-FDG-PET/CT检查的患者中,42.6%的患者影像学结果导致了后续诊断或治疗程序的改变。在29%的病例中,前哨淋巴结活检不再必要。F-FDG-PET/CT的敏感性和特异性分别为66.0%和93.0%。
全身成像作为主要诊断工具具有很高的价值,在相当数量肿瘤厚度相对较高的患者中影响后续诊断和治疗程序。它有助于避免多余前哨淋巴结活检的费用和侵入性,同时在诊断时加快患者的分期。