Mitsui Toko, Bando Yasuko K, Hirakawa Akihiro, Furusawa Kenji, Morimoto Ryota, Taguchi Eiji, Kimura Akira, Kamiya Haruo, Nishikimi Naomichi, Komori Kimihiro, Nishigami Kazuhiro, Murohara Toyoaki
Department of Cardiology, Nagoya University Graduate School of Medicine Nagoya Japan.
Meijo Hospital Nagoya Japan.
Circ Rep. 2023 Oct 17;5(11):405-414. doi: 10.1253/circrep.CR-23-0071. eCollection 2023 Nov 10.
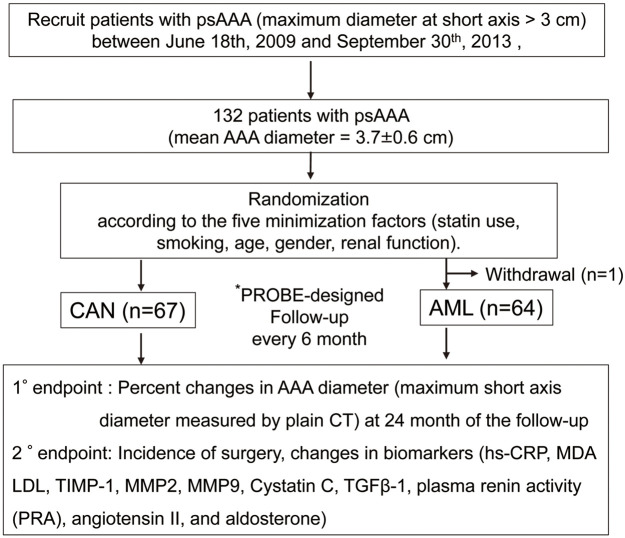
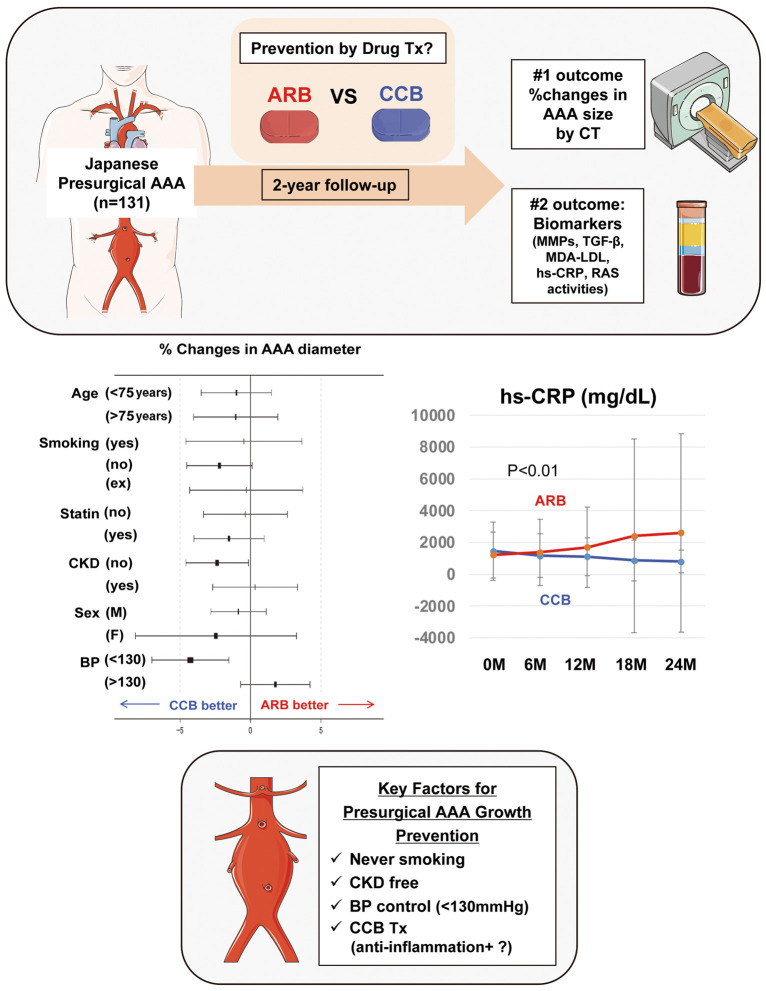
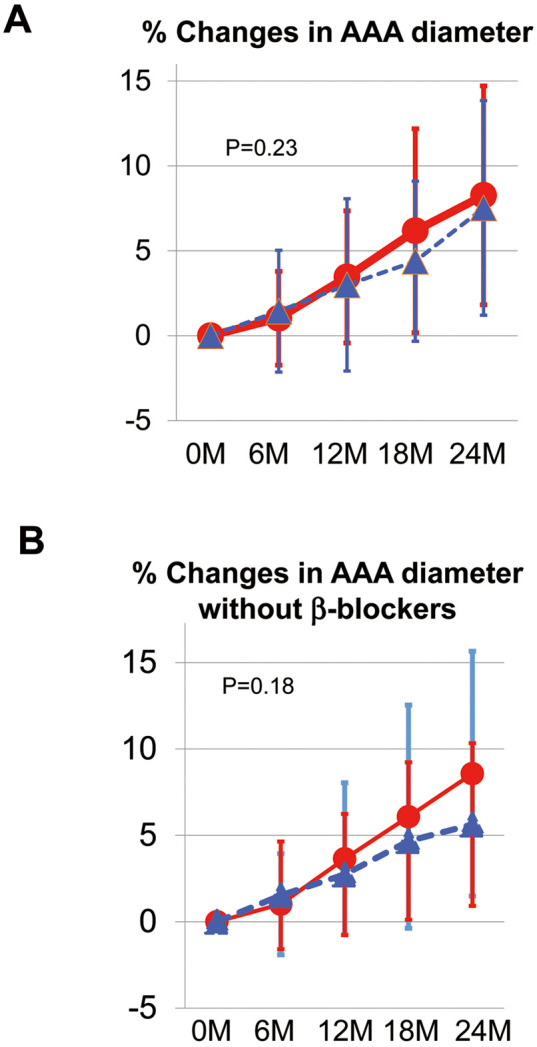
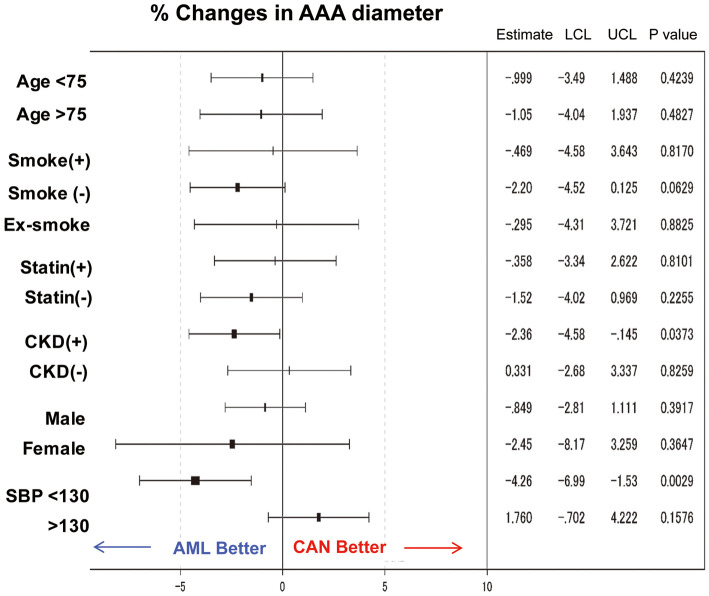
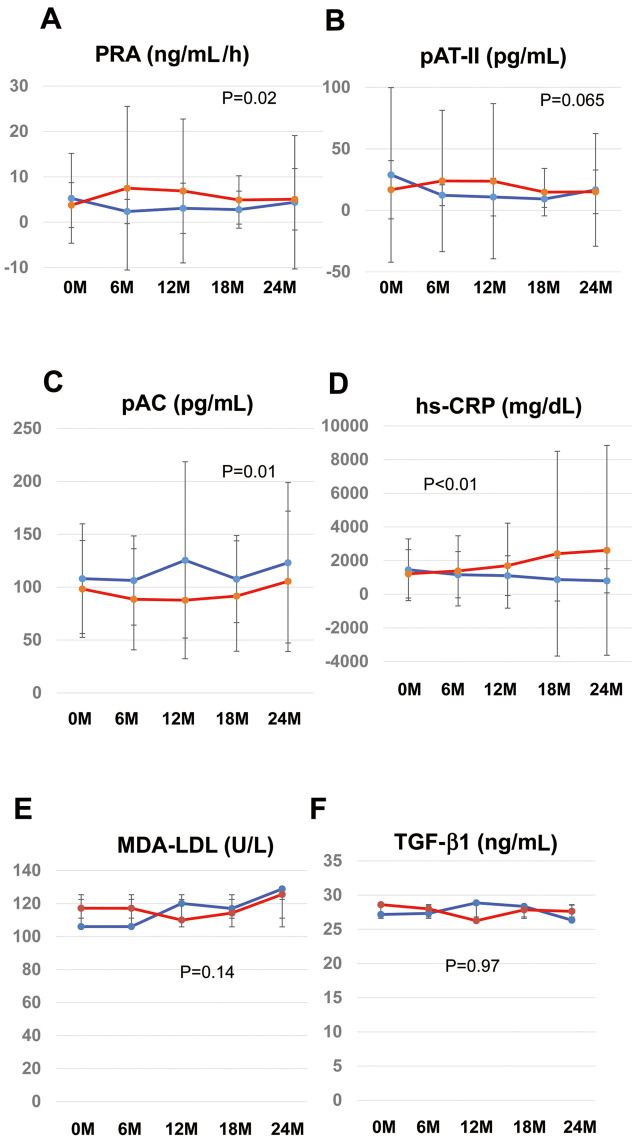
Whether drug therapy slows the growth of abdominal aortic aneurysms (AAAs) in the Japanese population remains unknown. In a multicenter prospective open-label study, patients with AAA at the presurgical stage (mean [±SD] AAA diameter 3.27±0.58 cm) were randomly assigned to treatment with candesartan (CAN; n=67) or amlodipine (AML; n=64) considering confounding factors (statin use, smoking, age, sex, renal function), with effects of blood pressure control minimized setting a target control level. The primary endpoint was percentage change in AAA diameter over 24 months. Secondary endpoints were changes in circulating biomarkers (high-sensitivity C-reactive protein [hs-CRP], malondialdehyde-low-density lipoprotein, tissue-specific inhibitor of metalloproteinase-1, matrix metalloproteinase [MMP] 2, MMP9, transforming growth factor-β1, plasma renin activity [PRA], angiotensin II, aldosterone). At 24 months, percentage changes in AAA diameter were comparable between the CAN and AML groups (8.4% [95% CI 6.23-10.59%] and 6.5% [95% CI 3.65-9.43%], respectively; P=0.23]. In subanalyses, AML attenuated AAA growth in patients with comorbid chronic kidney disease (CKD; P=0.04) or systolic blood pressure (SBP) <130 mmHg (P=0.003). AML exhibited a definite trend for slowing AAA growth exclusively in never-smokers (P=0.06). Among circulating surrogate candidates for AAA growth, PRA (P=0.02) and hs-CRP (P=0.001) were lower in the AML group. AML may prevent AAA growth in patients with CKD or lower SBP, associated with a decline in PRA and circulating hs-CRP.
药物治疗是否能减缓日本人群腹主动脉瘤(AAA)的生长尚不清楚。在一项多中心前瞻性开放标签研究中,将术前阶段的AAA患者(平均[±标准差]AAA直径3.27±0.58 cm)根据混杂因素(他汀类药物使用、吸烟、年龄、性别、肾功能)随机分配至坎地沙坦(CAN;n = 67)或氨氯地平(AML;n = 64)治疗组,并将血压控制效果最小化,设定目标控制水平。主要终点是24个月内AAA直径的百分比变化。次要终点是循环生物标志物(高敏C反应蛋白[hs-CRP]、丙二醛修饰低密度脂蛋白、金属蛋白酶组织抑制剂-1、基质金属蛋白酶[MMP]2、MMP9、转化生长因子-β1、血浆肾素活性[PRA]、血管紧张素II、醛固酮)的变化。在24个月时,CAN组和AML组的AAA直径百分比变化相当(分别为8.4%[95%CI 6.23 - 10.59%]和6.5%[95%CI 3.65 - 9.43%];P = 0.23)。在亚组分析中,AML可减缓合并慢性肾脏病(CKD;P = 0.04)或收缩压(SBP)<130 mmHg患者的AAA生长(P = 0.003)。AML仅在从不吸烟者中显示出减缓AAA生长的明确趋势(P = 0.06)。在AAA生长循环替代指标中,AML组的PRA(P = 0.02)和hs-CRP(P = 0.001)较低。AML可能预防CKD患者或SBP较低患者的AAA生长,这与PRA和循环hs-CRP下降有关。