Baldonado Jobelle J A R, Naffouje Samer A, Parvathaneni Sirish, Roy Esha, Toloza Eric M, Fontaine Jacques P
Department of Thoracic Oncology, Moffitt Cancer Center, Tampa, FL, USA.
Department of Gastrointestinal Oncology, Moffitt Cancer Center, Tampa, FL, USA.
J Thorac Dis. 2023 Oct 31;15(10):5349-5361. doi: 10.21037/jtd-22-1340. Epub 2023 Sep 22.
There continues to be a rise in the proportion of resectable non-small cell lung cancer (NSCLC) with the recent expansion of criteria for low-dose lung cancer screening. These are increasingly being treated with minimally invasive techniques. Our study aims to compare outcomes of robotic lobectomy (RL) for NSCLC at a National Cancer Institute-designated Comprehensive Cancer Center (NCI-CCC) to those of open lobectomy (OL), video-assisted thoracoscopic lobectomy (VL), or RL as reported in the National Cancer Database (NCDB).
The first 1,021 patients with NSCLC who underwent RL between 2010 and 2020 were matched with peers from the NCDB who had OL, VL, or RL. Matching was performed based on a propensity score calculated by logistic regression using multiple variables. Surgical outcomes included numbers of examined lymph nodes, performance of mediastinal lymphadenectomy, length of stay (LOS), and 30-day mortality. Kaplan-Meier curves and overall survival (OS) were analyzed using log-rank tests.
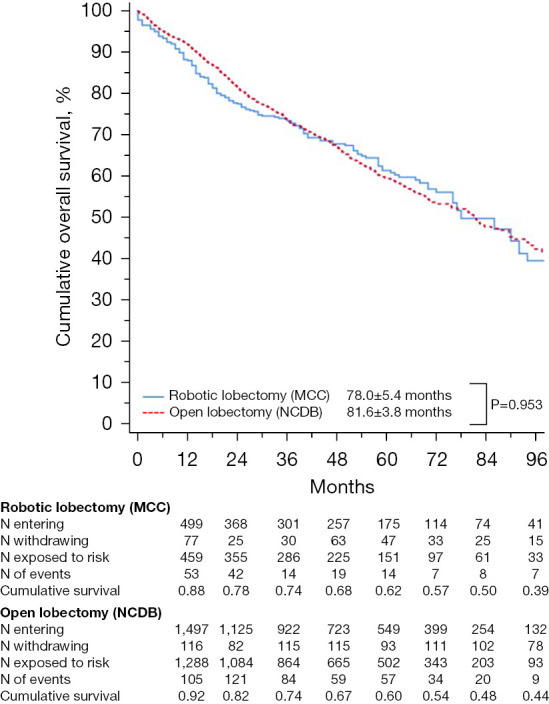
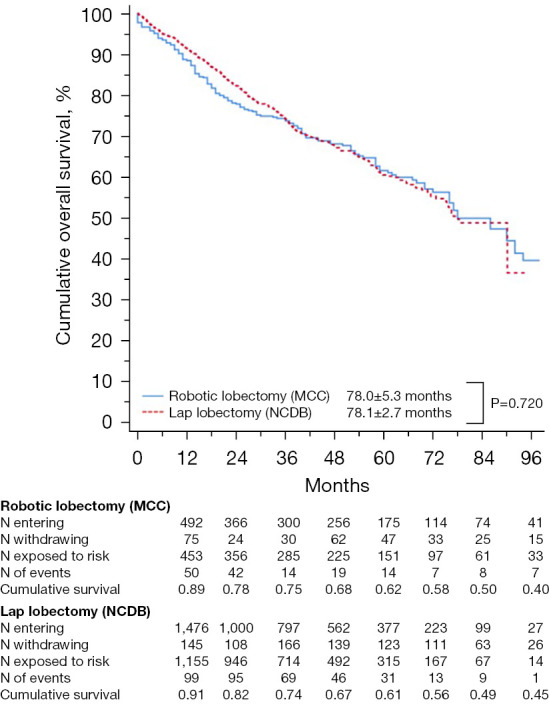
Most common postoperative complications were persistent air leak, atrial fibrillation, and pneumonia. Median LOS was 4 days, and the 30-day mortality rate was 1% (n=10/1,021). Compared to NCDB patients who underwent OL, NCI-CCC patients had a higher mean number of retrieved lymph nodes (P=0.001), higher rate of mediastinal lymphadenectomy (P<0.001), and shorter median LOS (4 6 days; P<0.001). There was no difference in 30-day mortality (P=0.176). Kaplan-Meier analyses showed no differences in median OS (log-rank P=0.953) or 5-year OS (P=0.774). Compared to NCDB VL, NCI-CCC patients had a higher nodal yield (P<0.001), higher rates of mediastinal lymphadenectomy (P<0.001), and lower conversion rates (4.1% 13.8%, P<0.001). There were no differences in 30-day mortality (P=0.379) or in median LOS (P=0.351). Kaplan-Meier analyses showed no differences in median OS (P=0.720) or 5-year OS (P=0.735). NCI-CCC patients were also matched with NCDB RL patients and had a higher nodal yield (P<0.001), higher rates of mediastinal lymphadenectomy (P<0.001), and lower conversion rates (4.1% 9.5%; P <0.001). There were no differences in 30-day mortality (P=0.899) or in median LOS (P=0.252). Kaplan-Meier analyses showed no differences in median OS (P=0.484) or 5-year OS (P=0.524).
RL for NSCLC performed in an NCI-CCC appears to have improved perioperative outcomes with comparable long-term OS compared to national benchmarks in OL and VL.
随着低剂量肺癌筛查标准最近的扩大,可切除非小细胞肺癌(NSCLC)的比例持续上升。这些患者越来越多地接受微创技术治疗。我们的研究旨在将一家国立癌症研究所指定的综合癌症中心(NCI-CCC)进行的NSCLC机器人肺叶切除术(RL)的结果与开放肺叶切除术(OL)、电视辅助胸腔镜肺叶切除术(VL)的结果,或国家癌症数据库(NCDB)中报告的RL结果进行比较。
2010年至2020年间接受RL的前1021例NSCLC患者与NCDB中接受OL、VL或RL的患者进行匹配。基于使用多个变量通过逻辑回归计算的倾向得分进行匹配。手术结果包括检查的淋巴结数量、纵隔淋巴结清扫术的执行情况、住院时间(LOS)和30天死亡率。使用对数秩检验分析Kaplan-Meier曲线和总生存期(OS)。
最常见的术后并发症是持续性漏气、心房颤动和肺炎。中位LOS为4天,30天死亡率为1%(n = 10/1021)。与接受OL的NCDB患者相比,NCI-CCC患者的平均回收淋巴结数量更多(P = 0.001),纵隔淋巴结清扫率更高(P < 0.001),中位LOS更短(4对6天;P < 0.001)。30天死亡率无差异(P = 0.176)。Kaplan-Meier分析显示中位OS(对数秩P = 0.953)或5年OS(P = 0.774)无差异。与NCDB的VL相比,NCI-CCC患者的淋巴结回收率更高(P < 0.001),纵隔淋巴结清扫率更高(P < 0.001),转化率更低(4.1%对13.8%,P < 0.001)。30天死亡率(P = 0.379)或中位LOS(P = 0.351)无差异。Kaplan-Meier分析显示中位OS(P = 0.720)或5年OS(P = 0.735)无差异。NCI-CCC患者也与NCDB的RL患者进行了匹配,淋巴结回收率更高(P < 0.001),纵隔淋巴结清扫率更高(P < 0.001),转化率更低(4.1%对9.5%;P < 0.001)。30天死亡率(P = 0.899)或中位LOS(P = 0.252)无差异。Kaplan-Meier分析显示中位OS(P = 0.484)或5年OS(P = 0.524)无差异。
在NCI-CCC进行的NSCLC的RL与OL和VL的全国基准相比,似乎改善了围手术期结果,长期OS相当。