González-Montero Jaime, Burotto Mauricio, Valenzuela Guillermo, Mateluna Debora, Buen-Abad Florencia, Toro Jessica, Barajas Olga, Marcelain Katherine
Bradford Hill Clinical Research Center, Santiago 8420383, Chile.
Basic and Clinical Oncology Department, University of Chile, Santiago 8380453, Chile.
World J Clin Oncol. 2023 Oct 24;14(10):409-419. doi: 10.5306/wjco.v14.i10.409.
Colorectal cancer is a complex disease with high mortality rates. Over time, the treatment of metastatic colorectal cancer (mCRC) has gradually improved due to the development of modern chemotherapy and targeted therapy regimens. However, due to the inherent heterogeneity of this condition, identifying reliable predictive biomarkers for targeted therapies remains challenging. A recent promising classification system-the consensus molecular subtype (CMS) system-offers the potential to categorize mCRC patients based on their unique biological and molecular characteristics. Four distinct CMS categories have been defined: immune (CMS1), canonical (CMS2), metabolic (CMS3), and mesenchymal (CMS4). Nevertheless, there is currently no standardized protocol for accurately classifying patients into CMS categories. To address this challenge, reverse transcription polymerase chain reaction (RT-qPCR) and next-generation genomic sequencing (NGS) techniques may hold promise for precisely classifying mCRC patients into their CMSs.
To investigate if mCRC patients can be classified into CMS categories using a standardized molecular biology workflow.
This observational study was conducted at the University of Chile Clinical Hospital and included patients with unresectable mCRC who were undergoing systemic treatment with chemotherapy and/or targeted therapy. Molecular biology techniques were employed to analyse primary tumour samples from these patients. RT-qPCR was utilized to assess the expression of genes associated with fibrosis (TGF-β and β-catenin) and cell growth pathways (c-MYC). NGS using a 25-gene panel (TumorSec) was performed to identify specific genomic mutations. The patients were then classified into one of the four CMS categories according to the clinical consensus of a Tumour Board. Informed consent was obtained from all the patients prior to their participation in this study. All techniques were conducted at University of Chile.
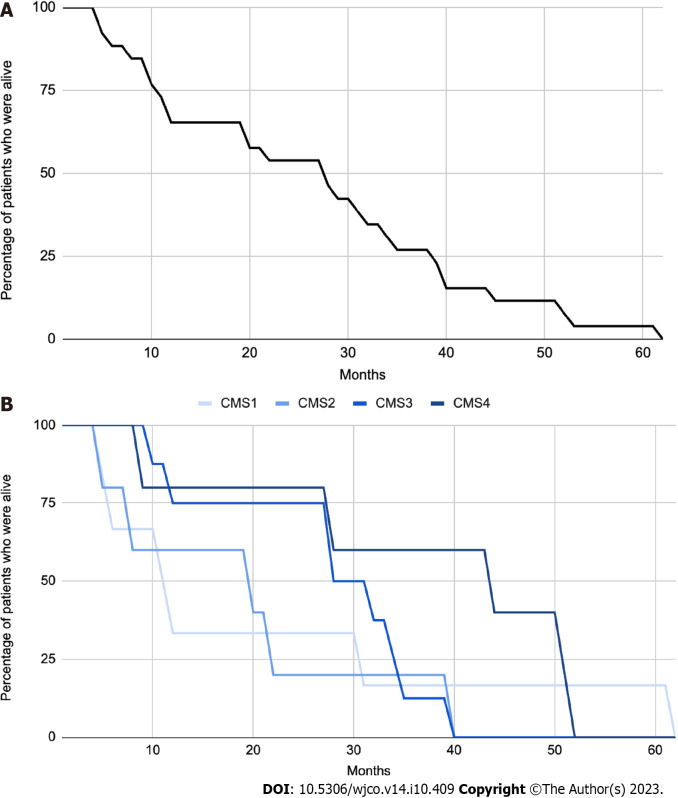
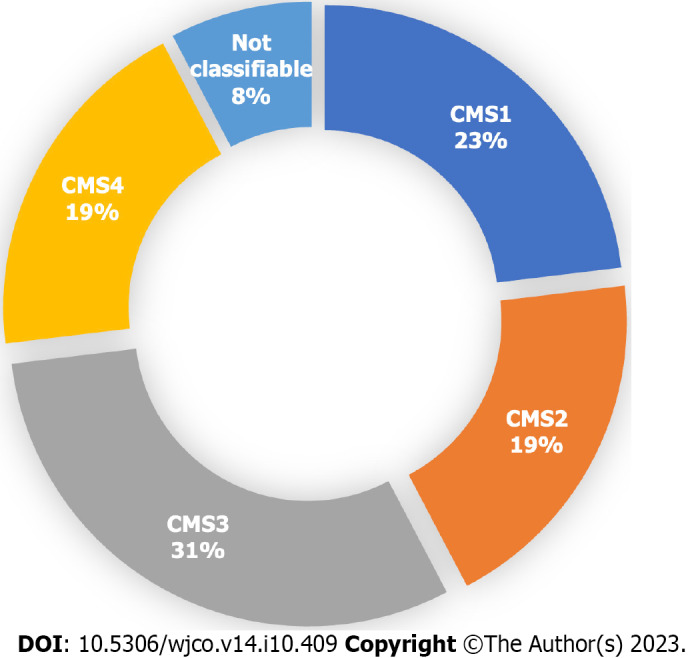
Twenty-six patients were studied with the techniques and then evaluated by the Tumour Board to determine the specific CMS. Among them, 23% ( = 6), 19% ( = 5), 31% ( = 8), and 19% ( = 5) were classified as CMS1, CMS2, CMS3, and CMS4, respectively. Additionally, 8% of patients ( = 2) could not be classified into any of the four CMS categories. The median overall survival of the total sample was 28 mo, and for CMS1, CMS2, CMS3 and CMS4 it was 11, 20, 30 and 45 mo respectively, with no statistically significant differences between groups.
A molecular biology workflow and clinical consensus analysis can be used to accurately classify mCRC patients. This classification process, which divides patients into the four CMS categories, holds significant potential for improving research strategies and targeted therapies tailored to the specific characteristics of mCRC.
结直肠癌是一种死亡率很高的复杂疾病。随着时间的推移,由于现代化疗和靶向治疗方案的发展,转移性结直肠癌(mCRC)的治疗逐渐得到改善。然而,由于这种疾病固有的异质性,识别用于靶向治疗的可靠预测生物标志物仍然具有挑战性。最近一种有前景的分类系统——共识分子亚型(CMS)系统——有望根据mCRC患者独特的生物学和分子特征对其进行分类。已定义了四种不同的CMS类别:免疫型(CMS1)、经典型(CMS2)、代谢型(CMS3)和间充质型(CMS4)。然而,目前尚无将患者准确分类到CMS类别的标准化方案。为应对这一挑战,逆转录聚合酶链反应(RT-qPCR)和下一代基因组测序(NGS)技术可能有望将mCRC患者精确分类到其相应的CMS类别中。
探讨能否使用标准化分子生物学工作流程将mCRC患者分类到CMS类别中。
这项观察性研究在智利大学临床医院进行,纳入了正在接受化疗和/或靶向治疗的不可切除mCRC患者。采用分子生物学技术分析这些患者的原发性肿瘤样本。利用RT-qPCR评估与纤维化相关基因(TGF-β和β-连环蛋白)以及细胞生长途径相关基因(c-MYC)的表达。使用25基因检测板(TumorSec)进行NGS以识别特定的基因组突变。然后根据肿瘤委员会的临床共识将患者分类到四种CMS类别之一。所有患者在参与本研究前均获得了知情同意。所有技术均在智利大学进行。
采用这些技术对26例患者进行了研究,然后由肿瘤委员会进行评估以确定具体的CMS。其中,分别有23%(=6)、19%(=5)、31%(=8)和19%(=5)被分类为CMS1、CMS2、CMS3和CMS4。此外,8%的患者(=2)无法分类到四种CMS类别中的任何一种。总样本的中位总生存期为28个月,CMS1、CMS2、CMS3和CMS4患者的中位总生存期分别为11、20、30和45个月,组间无统计学显著差异。
分子生物学工作流程和临床共识分析可用于准确分类mCRC患者。这种将患者分为四种CMS类别的分类过程,在改进针对mCRC特定特征的研究策略和靶向治疗方面具有巨大潜力。