Department of Laboratory Medicine and Pathobiology and Tanz Centre for Research in Neurodegenerative Disease, University of Toronto, Toronto, Ontario M5T 0S8, Canada.
Laboratory Medicine Program and Krembil Brain Institute, University Health Network, Toronto, Ontario M5T 0S8, Canada.
Brain. 2024 Apr 4;147(4):1399-1411. doi: 10.1093/brain/awad381.
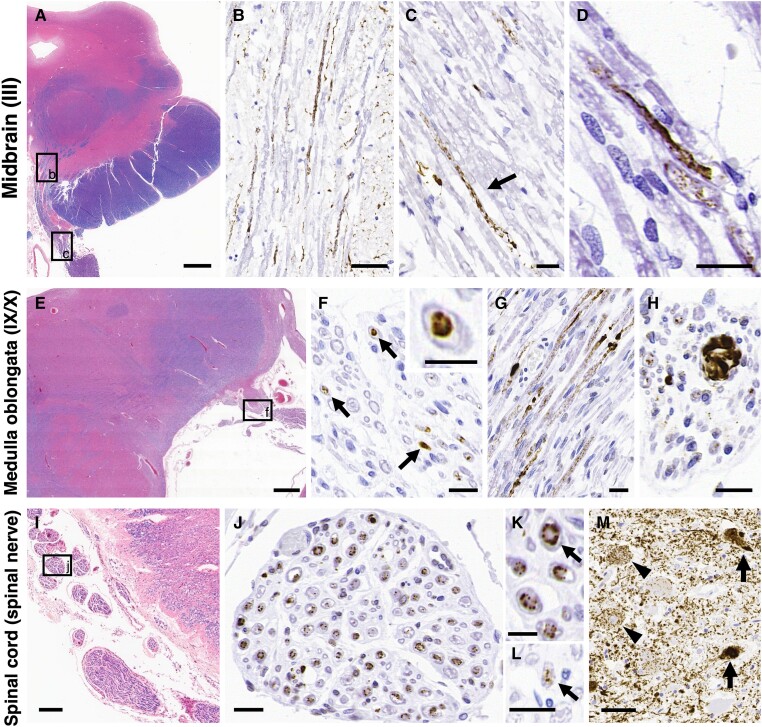
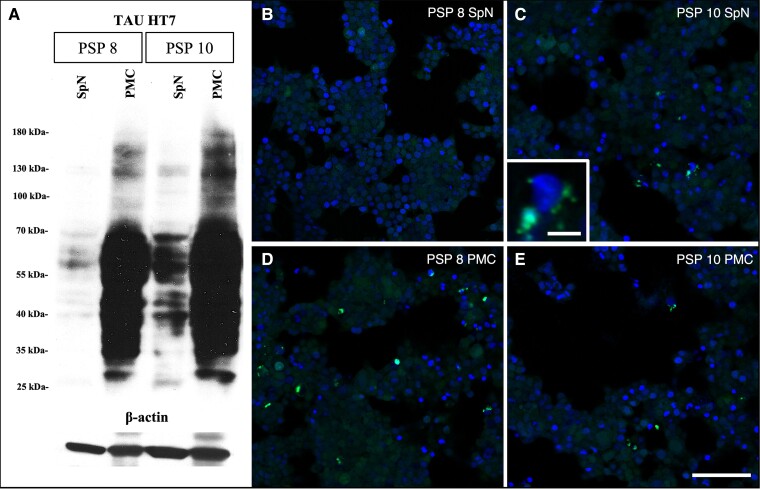
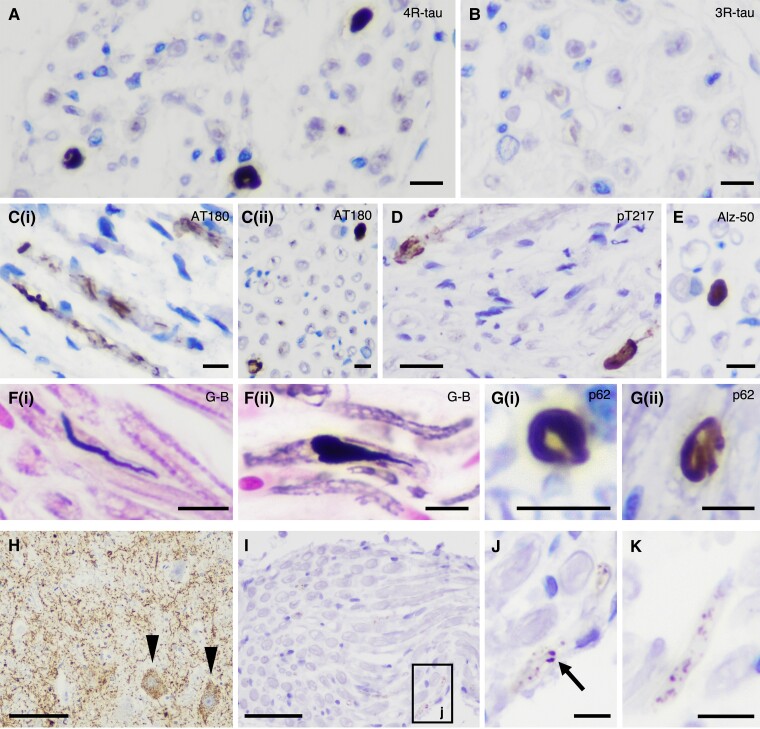
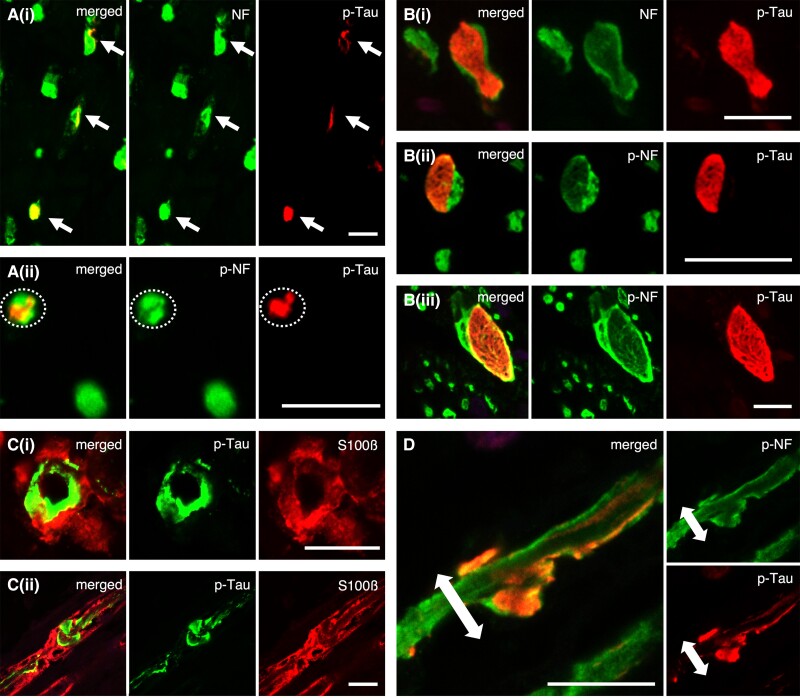
The most frequent neurodegenerative proteinopathies include diseases with deposition of misfolded tau or α-synuclein in the brain. Pathological protein aggregates in the PNS are well-recognized in α-synucleinopathies and have recently attracted attention as a diagnostic biomarker. However, there is a paucity of observations in tauopathies. To characterize the involvement of the PNS in tauopathies, we investigated tau pathology in cranial and spinal nerves (PNS-tau) in 54 tauopathy cases [progressive supranuclear palsy (PSP), n = 15; Alzheimer's disease (AD), n = 18; chronic traumatic encephalopathy (CTE), n = 5; and corticobasal degeneration (CBD), n = 6; Pick's disease, n = 9; limbic-predominant neuronal inclusion body 4-repeat tauopathy (LNT), n = 1] using immunohistochemistry, Gallyas silver staining, biochemistry, and seeding assays. Most PSP cases revealed phosphorylated and 4-repeat tau immunoreactive tau deposits in the PNS as follows: (number of tau-positive cases/available cases) cranial nerves III: 7/8 (88%); IX/X: 10/11 (91%); and XII: 6/6 (100%); anterior spinal roots: 10/10 (100%). The tau-positive inclusions in PSP often showed structures with fibrillary (neurofibrillary tangle-like) morphology in the axon that were also recognized with Gallyas silver staining. CBD cases rarely showed fine granular non-argyrophilic tau deposits. In contrast, tau pathology in the PNS was not evident in AD, CTE and Pick's disease cases. The single LNT case also showed tau pathology in the PNS. In PSP, the severity of PNS-tau involvement correlated with that of the corresponding nuclei, although, occasionally, p-tau deposits were present in the cranial nerves but not in the related brainstem nuclei. Not surprisingly, most of the PSP cases presented with eye movement disorder and bulbar symptoms, and some cases also showed lower-motor neuron signs. Using tau biosensor cells, for the first time we demonstrated seeding capacity of tau in the PNS. In conclusion, prominent PNS-tau distinguishes PSP from other tauopathies. The morphological differences of PNS-tau between PSP and CBD suggest that the tau pathology in PNS could reflect that in the central nervous system. The high frequency and early presence of tau lesions in PSP suggest that PNS-tau may have clinical and biomarker relevance.
最常见的神经退行性蛋白病变包括脑内错误折叠的 tau 或 α-突触核蛋白沉积的疾病。α-突触核蛋白病中已很好地认识到周围神经系统中的病理性蛋白聚集物,并且最近作为诊断生物标志物引起了关注。然而,在 tau 病中观察到的情况很少。为了描述 tau 病中周围神经系统的参与情况,我们研究了 54 例 tau 病病例(进行性核上性麻痹(PSP),n=15;阿尔茨海默病(AD),n=18;慢性创伤性脑病(CTE),n=5;皮质基底变性(CBD),n=6;Pick 病,n=9;边缘优势神经元包涵体 4 重复 tau 病(LNT),n=1)的颅神经和脊神经中的 tau 病理学(PNS-tau),使用免疫组织化学、Gallyas 银染色、生物化学和接种测定。大多数 PSP 病例在周围神经系统中显示出磷酸化和 4 重复 tau 免疫反应性 tau 沉积物,如下所示:(tau 阳性病例/可评估病例数)颅神经 III:7/8(88%);IX/X:10/11(91%);和 XII:6/6(100%);前脊神经根:10/10(100%)。PSP 中的 tau 阳性包涵体通常在轴突中显示出具有纤维状(神经原纤维缠结样)形态的结构,这些结构也通过 Gallyas 银染色识别。CBD 病例很少显示细颗粒非银染 tau 沉积物。相比之下,AD、CTE 和 Pick 病病例的 PNS-tau 病变不明显。唯一的 LNT 病例也显示出 PNS-tau 病变。在 PSP 中,PNS-tau 受累的严重程度与相应核的严重程度相关,尽管偶尔在颅神经中存在 p-tau 沉积物,但在相关脑核中不存在。不出所料,大多数 PSP 病例表现出眼球运动障碍和延髓症状,一些病例还表现出下运动神经元体征。使用 tau 生物传感器细胞,我们首次证明了 PNS 中的 tau 接种能力。总之,明显的 PNS-tau 将 PSP 与其他 tau 病区分开来。PSP 和 CBD 之间 PNS-tau 的形态差异表明,周围神经系统中的 tau 病理学可能反映中枢神经系统中的 tau 病理学。PSP 中 tau 病变的高频率和早期出现提示 PNS-tau 可能具有临床和生物标志物相关性。