RAND Corporation Santa Monica CA.
David Geffen School of Medicine at UCLA Los Angeles CA.
J Am Heart Assoc. 2023 Nov 21;12(22):e030653. doi: 10.1161/JAHA.123.030653. Epub 2023 Nov 20.
Black-White disparities in heart disease treatment may be attributable to differences in physician referral networks. We mapped physician networks for Medicare patients and examined within-physician Black-White differences in patient sharing between primary care physicians and cardiologists.
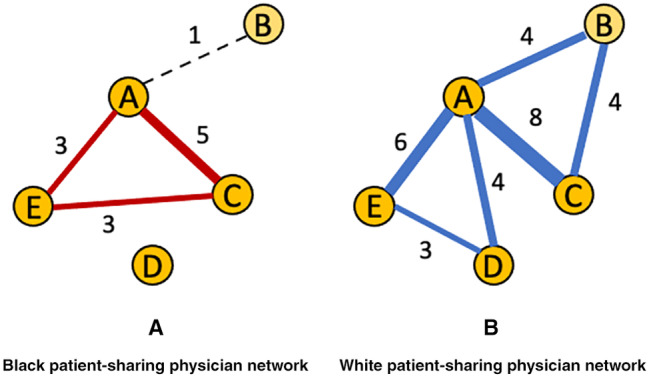
Using Medicare fee-for-service files for 2016 to 2017, we identified a cohort of Black and White patients with heart disease and the primary care physicians and cardiologists treating them. To ensure the robustness of within-physician comparisons, we restricted the sample to regional health care markets (ie, hospital referral regions) with at least 10 physicians sharing ≥3 Black and White patients. We used claims to construct 2 race-specific physician network measures: degree (number of cardiologists with whom a primary care physician shares patients) and transitivity (network tightness). Measures were adjusted for Black-White differences in physician panel size and calculated for all settings (hospital and office) and for office settings only. Of 306 US hospital referral regions, 226 and 145 met study criteria for all settings and office setting analyses, respectively. Black patients had more cardiology encounters overall (6.9 versus 6.6; <0.001) and with unique cardiologists (3.0 versus 2.6; <0.001), but fewer office encounters (31.7% versus 41.1%; <0.001). Primary care physicians shared Black patients with more cardiologists than White patients (mean differential degree 23.4 for all settings and 3.6 for office analyses; <0.001 for both). Black patient-sharing networks were less tightly connected in all but office settings (mean differential transitivity -0.2 for all settings [<0.001] and near 0 for office analyses [=0.74]).
Within-physician Black-White differences in patient sharing exist and may contribute to disparities in cardiac care.
心脏病治疗中的黑白差异可能归因于医生转诊网络的差异。我们绘制了医疗保险患者的医生网络,并检查了初级保健医生和心脏病专家之间患者共享的医生内黑白差异。
我们使用 2016 年至 2017 年的医疗保险按服务收费文件,确定了一组患有心脏病的黑人和白人患者以及为他们治疗的初级保健医生和心脏病专家。为了确保医生内比较的稳健性,我们将样本限制在至少有 10 名医生共享≥3 名黑人和白人患者的区域医疗保健市场(即医院转诊区域)。我们使用索赔来构建 2 个特定种族的医生网络指标:度(与初级保健医生共享患者的心脏病专家数量)和转导(网络紧密度)。这些措施根据医生小组规模的黑白差异进行了调整,并在所有环境(医院和办公室)以及仅在办公室环境中进行了计算。在 306 个美国医院转诊区域中,分别有 226 个和 145 个满足所有环境和办公室环境分析的研究标准。黑种人总体上接受的心脏病学治疗更多(6.9 次与 6.6 次;<0.001),且与独特的心脏病专家接触更多(3.0 次与 2.6 次;<0.001),但办公室就诊次数更少(31.7%与 41.1%;<0.001)。与白人患者相比,初级保健医生与更多的心脏病专家共享黑人患者(所有环境下的平均差异度为 23.4,办公室分析为 3.6;均<0.001)。除了办公室环境外,黑人患者的共享网络连接性都较差(所有环境的平均差异转导为-0.2 [<0.001],而办公室分析接近 0 [=0.74])。
医生内的黑人-白人患者共享存在差异,这可能导致心脏护理方面的差异。