Laurikkala Johanna, Ameloot Koen, Reinikainen Matti, Palmers Pieter-Jan, De Deyne Cathy, Bert Ferdinande, Dupont Matthias, Janssens Stefan, Dens Joseph, Hästbacka Johanna, Jakkula Pekka, Loisa Pekka, Birkelund Thomas, Wilkman Erika, Vaara Suvi T, Skrifvars Markus B
Department of Anaesthesiology, Intensive Care and Pain Medicine, Helsinki University Hospital and University of Helsinki, Haartmaninkatu 9, 00290 HUS, Helsinki, Finland.
Department of Cardiology, Ziekenhuis Oost-Limburg, Genk, Belgium.
Ann Intensive Care. 2023 Nov 21;13(1):113. doi: 10.1186/s13613-023-01210-0.
We aimed to study the incidence of acute kidney injury (AKI) in out-of-hospital cardiac arrest (OHCA) patients treated according to low-normal or high-normal mean arterial pressure (MAP) targets.
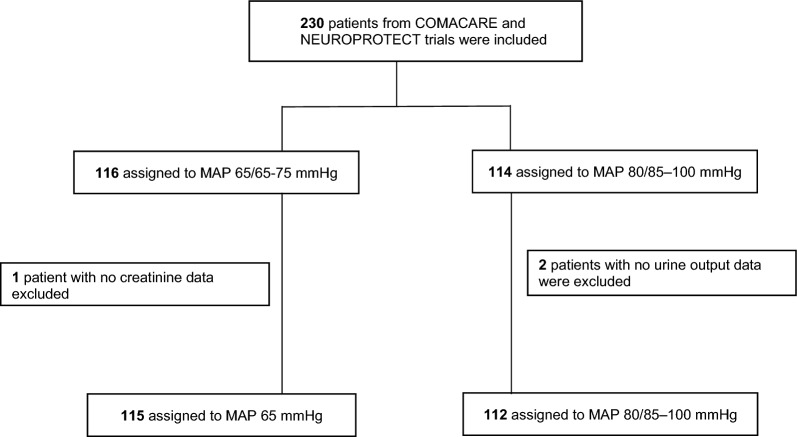
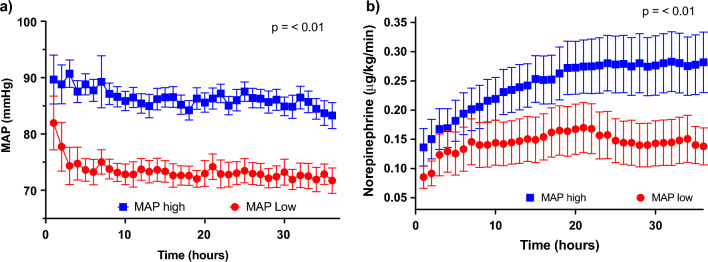
A post hoc analysis of the COMACARE (NCT02698917) and Neuroprotect (NCT02541591) trials that randomized patients to lower or higher targets for the first 36 h of intensive care. Kidney function was defined using the Kidney Disease Improving Global Outcome (KDIGO) classification. We used Cox regression analysis to identify factors associated with AKI after OHCA.
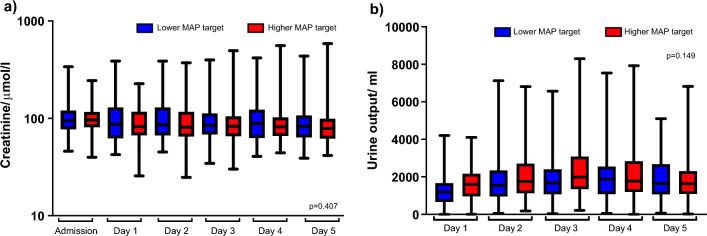
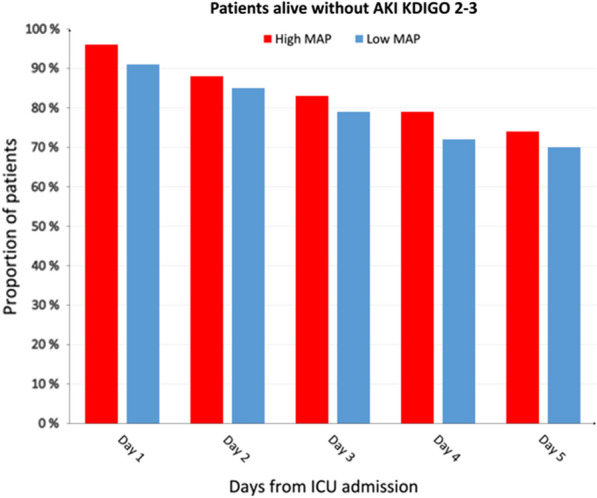
A total of 227 patients were included: 115 in the high-normal MAP group and 112 in the low-normal MAP group. Eighty-six (38%) patients developed AKI during the first five days; 40 in the high-normal MAP group and 46 in the low-normal MAP group (p = 0.51). The median creatinine and daily urine output were 85 μmol/l and 1730 mL/day in the high-normal MAP group and 87 μmol/l and 1560 mL/day in the low-normal MAP group. In a Cox regression model, independent AKI predictors were no bystander cardiopulmonary resuscitation (p < 0.01), non-shockable rhythm (p < 0.01), chronic hypertension (p = 0.03), and time to the return of spontaneous circulation (p < 0.01), whereas MAP target was not an independent predictor (p = 0.29).
Any AKI occurred in four out of ten OHCA patients. We found no difference in the incidence of AKI between the patients treated with lower and those treated with higher MAP after CA. Higher age, non-shockable initial rhythm, and longer time to ROSC were associated with shorter time to AKI.
COMACARE (NCT02698917), NEUROPROTECT (NCT02541591).
我们旨在研究根据平均动脉压(MAP)目标为低正常或高正常水平治疗的院外心脏骤停(OHCA)患者中急性肾损伤(AKI)的发生率。
对COMACARE(NCT02698917)和Neuroprotect(NCT02541591)试验进行事后分析,这些试验将患者随机分为在重症监护的前36小时采用较低或较高目标。使用改善全球肾脏病预后(KDIGO)分类来定义肾功能。我们使用Cox回归分析来确定OHCA后与AKI相关的因素。
共纳入227例患者:高正常MAP组115例,低正常MAP组112例。86例(38%)患者在头五天内发生AKI;高正常MAP组40例,低正常MAP组46例(p = 0.51)。高正常MAP组的肌酐中位数和每日尿量分别为85μmol/l和1730 mL/天,低正常MAP组分别为87μmol/l和1560 mL/天。在Cox回归模型中,AKI的独立预测因素为无旁观者心肺复苏(p < 0.01)、不可电击心律(p < 0.01)、慢性高血压(p = 0.03)以及自主循环恢复时间(p < 0.01),而MAP目标不是独立预测因素(p = 0.29)。
十分之四的OHCA患者发生了任何AKI。我们发现心脏骤停后接受较低MAP治疗的患者与接受较高MAP治疗的患者之间AKI发生率没有差异。年龄较大、初始心律不可电击以及自主循环恢复时间较长与AKI发生时间较短相关。
COMACARE(NCT02698917),NEUROPROTECT(NCT02541591)。