Grange Rémi, Di Bisceglie Mathieu, Habert Paul, Resseguier Noémie, Sarkissian Robin, Ferre Marjorie, Dassa Michael, Grange Sylvain, Izaaryene Jean, Piana Gilles
Department of Interventional Radiology, University Hospital of Saint-Etienne, University Hospital of Saint-Etienne, Avenue Albert Raimond, 42270, Saint-Priest-en-Jarez, France.
Department of Interventional Radiology, Institut Paoli Calmettes, Marseille, France.
Insights Imaging. 2023 Nov 28;14(1):212. doi: 10.1186/s13244-023-01566-8.
To evaluate the effect of tract embolization (TE) with gelatin sponge slurries during a percutaneous lung biopsy on chest tube placement and to evaluate the predictive factors of chest tube placement.
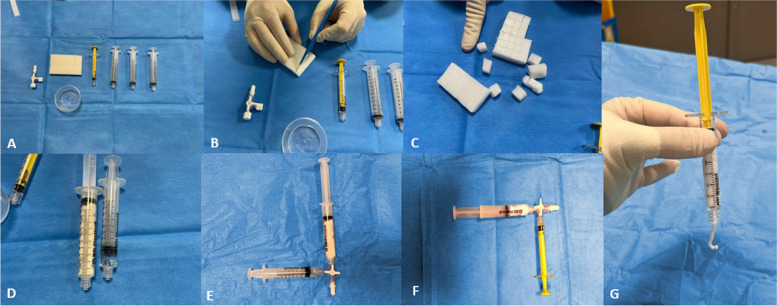
Percutaneous CT-guided lung biopsies performed with (TE) or without (non-TE) tract embolization or between June 2012 and December 2021 at three referral tertiary centers were retrospectively analyzed. The exclusion criteria were mediastinal biopsies, pleural tumors, and tumors adjacent to the pleura without pleural crossing. Variables related to patients, tumors, and procedures were collected. Univariable and multivariable analyses were performed to determine risk factors for chest tube placement. Furthermore, the propensity score matching analysis was adopted to yield a matched cohort.
A total of 1157 procedures in 1157 patients were analyzed, among which 560 (48.4%) were with TE (mean age 66.5 ± 9.2, 584 men). The rates of pneumothorax (44.9% vs. 26.1%, respectively; p < 0.001) and chest tube placement (4.8% vs. 2.3%, respectively; p < 0.001) were significantly higher in the non-TE group than in the TE group. No non-targeted embolization or systemic air embolism occurred. In the whole population, two protective factors for chest tube placement were found in univariate analysis: TE (OR 0.465 [0.239-0.904], p < 0.05) and prone position (OR 0.212 [0.094-0.482], p < 0.001). These data were confirmed in multivariate analysis (p < 0.001 and p < 0.0001 respectively). In the propensity matched cohort, TE reduces significatively the risk of chest tube insertion (OR = 0.44 [0.21-0.87], p < 0.05).
The TE technique using standardized gelatin sponge slurry reduces the need for chest tube placement after percutaneous CT-guided lung biopsy.
The tract embolization technique using standardized gelatin sponge slurry reduces the need for chest tube placement after percutaneous CT-guided lung biopsy.
评估经皮肺活检期间使用明胶海绵混悬液进行针道栓塞(TE)对胸腔闭式引流管放置的影响,并评估胸腔闭式引流管放置的预测因素。
回顾性分析2012年6月至2021年12月在三家转诊三级中心进行的经CT引导的经皮肺活检,分为使用(TE)或不使用(非TE)针道栓塞组。排除标准为纵隔活检、胸膜肿瘤以及未穿过胸膜的胸膜旁肿瘤。收集与患者、肿瘤和手术相关的变量。进行单因素和多因素分析以确定胸腔闭式引流管放置的危险因素。此外,采用倾向评分匹配分析以产生匹配队列。
共分析了1157例患者的1157例手术,其中560例(48.4%)采用TE(平均年龄66.5±9.2岁,男性584例)。非TE组气胸发生率(分别为44.9%和26.1%;p<0.001)和胸腔闭式引流管放置率(分别为4.8%和2.3%;p<0.001)显著高于TE组。未发生非靶向栓塞或全身性空气栓塞。在总体人群中,单因素分析发现胸腔闭式引流管放置的两个保护因素:TE(OR 0.465[0.239 - 0.904],p<0.05)和俯卧位(OR 0.212[0.094 - 0.482],p<0.001)。多因素分析证实了这些数据(分别为p<0.001和p<0.0001)。在倾向匹配队列中,TE显著降低了胸腔闭式引流管插入的风险(OR = 0.44[0.21 - 0.87],p<0.05)。
使用标准化明胶海绵混悬液的TE技术可减少经CT引导的经皮肺活检后胸腔闭式引流管的放置需求。
使用标准化明胶海绵混悬液的针道栓塞技术可减少经CT引导的经皮肺活检后胸腔闭式引流管的放置需求。