Wong Edwin, Nester Carla, Cavero Teresa, Karras Alexandre, Le Quintrec Moglie, Lightstone Liz, Eisenberger Ute, Soler Maria Jose, Kavanagh David, Daina Erica, Praga Manuel, Medjeral-Thomas Nicholas R, Gäckler Anja, Garcia-Carro Clara, Biondani Andrea, Chaperon Frederique, Kulmatycki Kenneth, Milojevic Julie, Webb Nicholas J A, Nidamarthy Prasanna Kumar, Junge Guido, Remuzzi Giuseppe
National Renal Complement Therapeutics Centre, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, UK.
Translational and Clinical Research Institute, Newcastle University, Newcastle Upon Tyne, UK.
Kidney Int Rep. 2023 Sep 22;8(12):2754-2764. doi: 10.1016/j.ekir.2023.09.017. eCollection 2023 Dec.
Complement 3 glomerulopathy (C3G) is a rare inflammatory kidney disease mediated by dysregulation of the alternative complement pathway. No targeted therapy exists for this aggressive glomerulonephritis. Efficacy, safety, tolerability, pharmacokinetics (PK), and pharmacodynamics (PD) (measured by complement biomarkers) of iptacopan were assessed in patients with C3G.
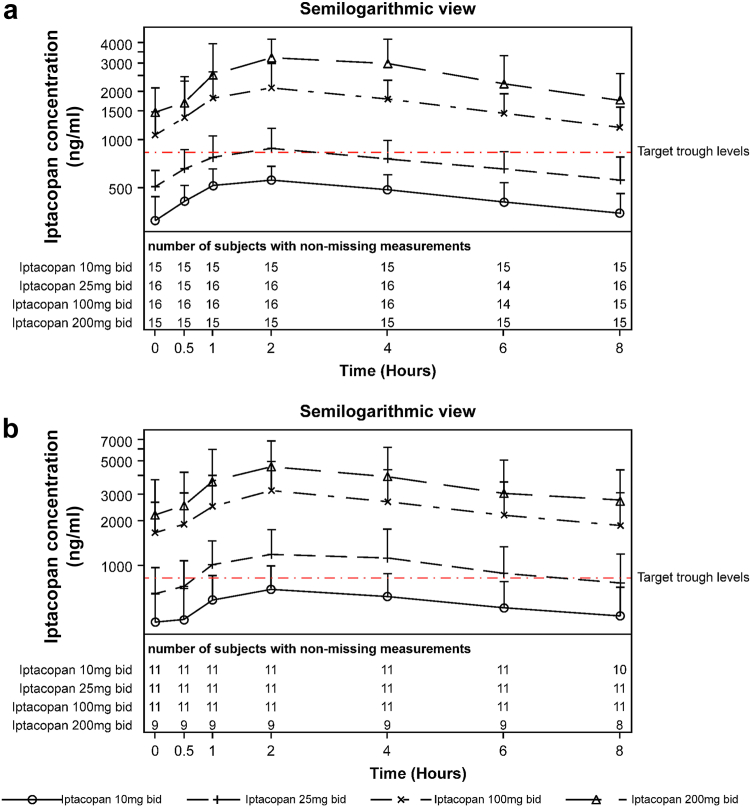
In this phase 2, multicenter, open-label, single-arm, nonrandomized study, adults with biopsy-proven, native kidney C3G (native cohort) and kidney transplant recipients with C3G recurrence (recurrent kidney transplant [KT] cohort) received iptacopan twice daily (bid) for 84 days (days 1-21: 10-100 mg; days 22-84: 200 mg). The primary end point was the urine protein-to-creatinine ratio (UPCR; native cohort) and the change in the C3 deposit score of kidney biopsy (recurrent KT cohort). The complement pathway measures included Wieslab assay, soluble C5b9, and serum C3 levels.
A total of 27 patients (16 native cohort and 11 recurrent KT cohort) were enrolled and all completed the study. In the native cohort, UPCR levels decreased by 45% from baseline to week 12 ( = 0.0003). In the recurrent KT cohort, the median C3 deposit score decreased by 2.50 (scale: 0-12) on day 84 versus baseline ( = 0.03). Serum C3 levels were normalized in most patients; complement hyperactivity observed pretreatment was reduced. Severe adverse events (AEs) included post-biopsy hematuria and hyperkalemia. No deaths occurred during the study.
Iptacopan resulted in statistically significant and clinically important reductions in UPCR and normalization of serum C3 levels in the native cohort and reduced C3 deposit scores in the recurrent KT cohort with favorable safety and tolerability. (ClinicalTrials.gov identifier: NCT03832114).
补体3肾小球病(C3G)是一种罕见的炎症性肾脏疾病,由替代补体途径失调介导。目前尚无针对这种侵袭性肾小球肾炎的靶向治疗方法。本研究评估了iptacopan在C3G患者中的疗效、安全性、耐受性、药代动力学(PK)和药效学(PD)(通过补体生物标志物测量)。
在这项2期、多中心、开放标签、单臂、非随机研究中,经活检证实患有原发性肾脏C3G的成人(原发性队列)和C3G复发的肾移植受者(复发性肾移植[KT]队列)每天接受两次iptacopan治疗,持续84天(第1 - 21天:10 - 100毫克;第22 - 84天:200毫克)。主要终点是尿蛋白与肌酐比值(UPCR;原发性队列)以及肾活检C3沉积评分的变化(复发性KT队列)。补体途径指标包括Wieslab检测、可溶性C5b9和血清C3水平。
共纳入27例患者(16例原发性队列和11例复发性KT队列),所有患者均完成研究。在原发性队列中,UPCR水平从基线到第12周下降了45%(P = 0.0003)。在复发性KT队列中,第84天的C3沉积评分中位数与基线相比下降了2.50(范围:0 - 12)(P = 0.03)。大多数患者的血清C3水平恢复正常;治疗前观察到的补体过度激活有所减轻。严重不良事件(AE)包括活检后血尿和高钾血症。研究期间无死亡病例。
Iptacopan在原发性队列中导致UPCR有统计学意义的显著降低和血清C3水平正常化,在复发性KT队列中降低了C3沉积评分,且安全性和耐受性良好。(ClinicalTrials.gov标识符:NCT03832114)