Ohkubo Maki, Fukuda Kuniaki, Chiba Shigeru, Homma Masato
Department of Pharmacy, University of Tsukuba Hospital, Ibaraki, Japan.
Department of Pharmaceutical Sciences, Graduate School of Comprehensive Human Sciences, University of Tsukuba, Ibaraki, Japan.
J Pharm Health Care Sci. 2023 Dec 19;9(1):52. doi: 10.1186/s40780-023-00321-x.
Nucleoside analogues (NAs) such as entecavir are required for at least 12 months when patients with resolved hepatitis B virus (HBV) infection develop HBV reactivation. Entecavir treatment does not always achieve hepatitis B surface antigen (HBsAg) seroconversion. The cessation of NA for HBV reactivation sometimes causes HBV rebound. The impact of hepatitis B core-related antigen (HBcrAg) on predicting HBV rebound is controversial.
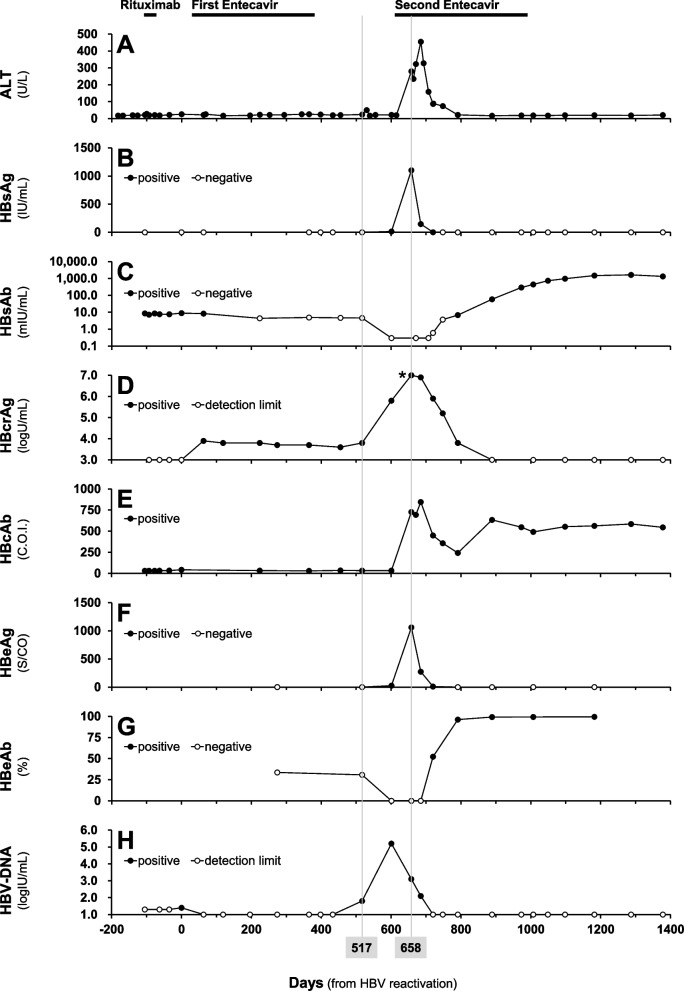
A 67-year-old woman with resolved HBV infection received rituximab for post-transplant lymphoproliferative disorder after peripheral blood stem cell transplantation. Since she tested positive for HBV-DNA after the first rituximab therapy (day 0), entecavir treatment was started. Because the HBV-DNA test became negative and her liver function had been normal, entecavir was terminated on day 376. According to the retrospective measurements, HBcrAg remained positive while the HBV-DNA level was undetectable. One hundred forty-one days after entecavir cessation, the HBV-DNA turned positive again, suggesting HBV rebound (day 517). Her liver function deteriorated and HBV infection worsened, even though entecavir treatment was resumed on day 615. On the contrary, hepatitis B surface antibody levels increased after the rebound, resulting in HBsAg seroconversion with HBcrAg and HBV-DNA levels undetectable. HBV reactivation has not been detected after the second entecavir cessation, and both HBcrAg and HBV-DNA levels remained undetectable.
This case suggests that NA cessation induced-HBV rebound achieved HBsAg seroconversion under the guidance of a hepatologist. Since HBcrAg had been detectable while HBV-DNA was undetectable, HBcrAg may be an index for predicting HBV rebound resulting in HBsAg seroconversion as well as other conventional laboratory tests. Prospective measuring HBcrAg is required to confirm this case report.
对于乙肝病毒(HBV)感染已缓解的患者发生HBV再激活时,恩替卡韦等核苷类似物(NAs)治疗至少需要12个月。恩替卡韦治疗并不总能实现乙肝表面抗原(HBsAg)血清学转换。因HBV再激活停用核苷类似物有时会导致HBV反弹。乙肝核心相关抗原(HBcrAg)对预测HBV反弹的影响存在争议。
一名67岁的女性,其HBV感染已缓解,在接受外周血干细胞移植后因移植后淋巴细胞增殖性疾病接受利妥昔单抗治疗。由于她在首次利妥昔单抗治疗后(第0天)HBV-DNA检测呈阳性,遂开始恩替卡韦治疗。因HBV-DNA检测变为阴性且肝功能一直正常,恩替卡韦于第376天停用。根据回顾性检测,在HBV-DNA水平不可检测时,HBcrAg仍为阳性。停用恩替卡韦141天后,HBV-DNA再次转为阳性,提示HBV反弹(第517天)。尽管在第615天恢复了恩替卡韦治疗,但其肝功能恶化且HBV感染加重。相反,反弹后乙肝表面抗体水平升高,导致HBsAg血清学转换,此时HBcrAg和HBV-DNA水平均不可检测。第二次停用恩替卡韦后未检测到HBV再激活,HBcrAg和HBV-DNA水平均保持不可检测。
该病例表明,在肝病专家的指导下,因停用核苷类似物诱导的HBV反弹实现了HBsAg血清学转换。由于在HBV-DNA不可检测时HBcrAg仍可检测到,HBcrAg可能是预测导致HBsAg血清学转换的HBV反弹以及其他传统实验室检查的一个指标。需要进行前瞻性检测HBcrAg以证实本病例报告。