Mondal R, Maitra A, Saha S, Deb S, Roy A G, Mahata M, Lahiri D, Benito-León J
Department of Clinical Pharmacology and Therapeutic Medicine, IPGMER and SSKM Hospital, Kolkata, India.
Department of Cardiology, Bellevue clinic, Kolkata, India.
Neurol Perspect. 2023 Oct-Dec;3(4). doi: 10.1016/j.neurop.2023.100134. Epub 2023 Oct 4.
Obstructive sleep apnea is a highly prevalent disorder, characterized by recurrent events of upper airway obstruction during sleep and associated with recurrent cycles of desaturation and re-oxygenation, sympathetic hyperactivity, and intra-thoracic pressure fluctuations, resulting in fragmentation of sleep and subsequent daytime fatigue with excessive sleepiness. Obstructive sleep apnea-induced bilateral tonic-clonic seizures are unheard of. We aimed to report 3 patients with previously undiagnosed obstructive sleep apnea who presented to the emergency department with new onset bilateral tonic-clonic seizure without any evidential neurological or metabolic cause.
Patient data were obtained from medical records from the Department of Internal Medicine, IPGMER and SSKM Hospital, Kolkata, and Belle Vue Clinic, Kolkata, India.
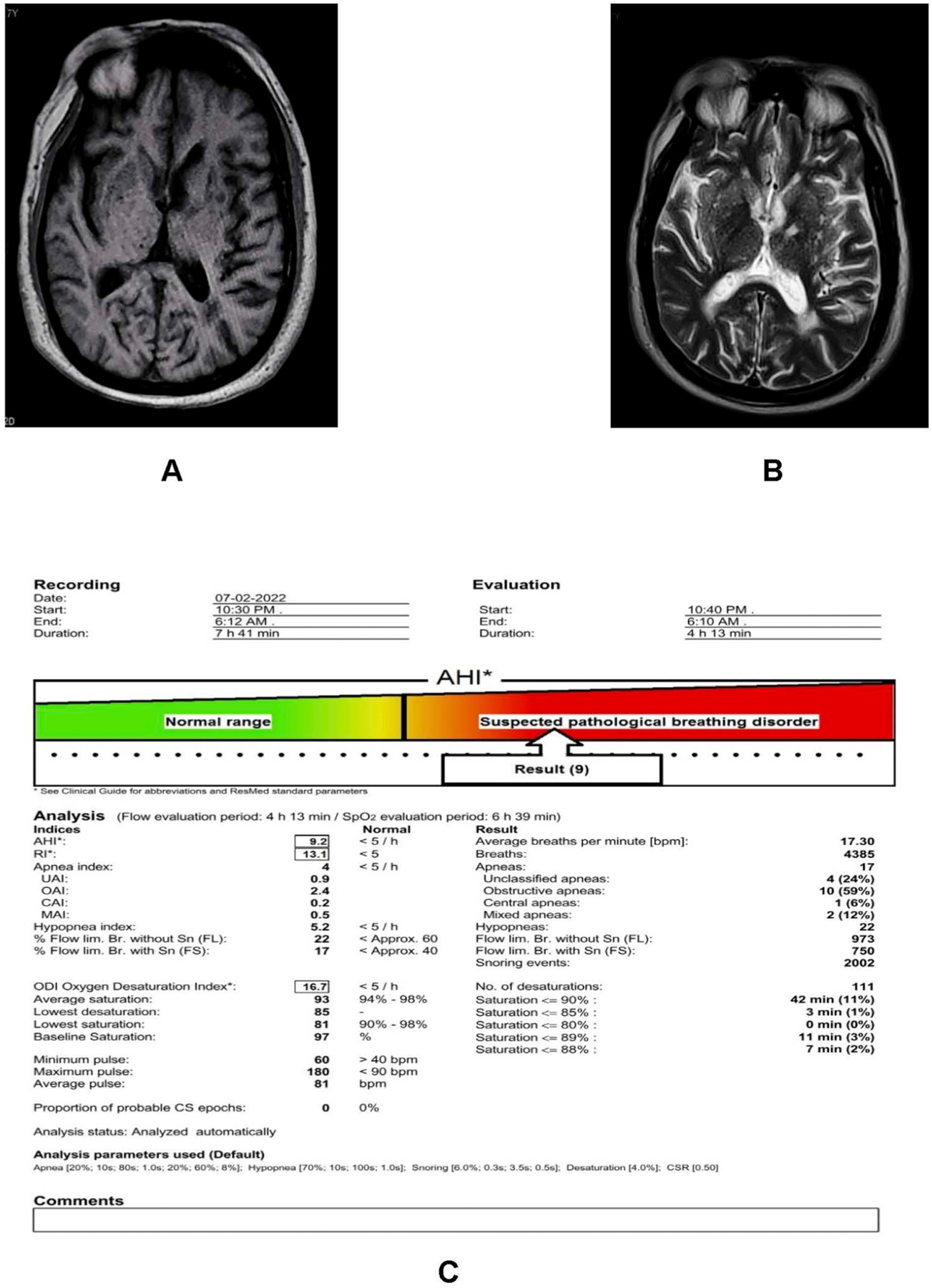
Three male patients (67, 58, and 44 years old) presented with bilateral tonic-clonic seizure disorder without any underlying cause of seizures after rigorous investigations except for moderate to severe obstructive sleep apnea on polysomnography. All 2 patients were seizure-free after being treated with levetiracetam, chronic continuous positive airway pressure therapy in 2, and only continuous positive airway pressure in the other. The patients remained seizure-free on continuous positive airway pressure, even when levetiracetam was withdrawn, suggesting obstructive sleep apnea's causality in their new-onset acute seizures.
Although further investigation is required to clarify this association, underlying obstructive sleep apnea should be ruled out in patients with a first-ever bilateral tonic-clonic seizure. Whether or not continuous positive airway pressure alone could effectively treat hypoxia and deranged cortical excitability, which may lead to seizures in cases with longstanding obstructive sleep apnea, is yet to be explored.
阻塞性睡眠呼吸暂停是一种高度流行的疾病,其特征为睡眠期间上气道反复阻塞,并伴有反复的血氧饱和度下降和再氧合、交感神经过度活跃以及胸内压力波动,导致睡眠碎片化以及随后出现日间疲劳和过度嗜睡。阻塞性睡眠呼吸暂停诱发的双侧强直阵挛性癫痫发作尚无报道。我们旨在报告3例先前未诊断出阻塞性睡眠呼吸暂停的患者,他们因新发双侧强直阵挛性癫痫发作就诊于急诊科,且无任何神经学或代谢方面的病因证据。
患者数据来自印度加尔各答IPGMER和SSKM医院内科以及加尔各答贝尔维尤诊所的病历。
3例男性患者(年龄分别为67岁、58岁和44岁)出现双侧强直阵挛性癫痫发作,在进行严格检查后,除多导睡眠图显示中度至重度阻塞性睡眠呼吸暂停外,未发现癫痫发作的任何潜在病因。所有3例患者中,2例接受左乙拉西坦治疗,2例接受慢性持续气道正压通气治疗,另1例仅接受持续气道正压通气治疗,之后均未再发作。即使停用左乙拉西坦,患者在持续气道正压通气治疗下仍未再发作,提示阻塞性睡眠呼吸暂停与他们新发的急性癫痫发作存在因果关系。
尽管需要进一步研究来阐明这种关联,但首次出现双侧强直阵挛性癫痫发作的患者应排除潜在的阻塞性睡眠呼吸暂停。持续气道正压通气单独是否能有效治疗缺氧和紊乱的皮质兴奋性(这可能导致长期阻塞性睡眠呼吸暂停患者发生癫痫发作),仍有待探索。