Coronary Heart Disease Center, Department of Cardiology, Fuwai Hospital, CAMS&PUMC. No.167 North Lishi Road, Xicheng District, Beijing, China.
People's Hospital of Bayingoleng Mongolian Autonomous Prefecture, No. 56, Renmin East Road, Korla City, Bayingoleng Mongolian Autonomous Prefecture, Xinjiang Uygur Autonomous Region, China.
BMC Cardiovasc Disord. 2024 Jan 2;24(1):3. doi: 10.1186/s12872-023-03678-x.
Aslanger's pattern in electrocardiogram (ECG) indicates that patients may have acute inferior myocardial infarction(AMI) with concomitant critical stenoses on other coronary arteries, which needs to be evaluated the timing of revascularization as risk equivalents of ST elevation myocardial infarction(STEMI).
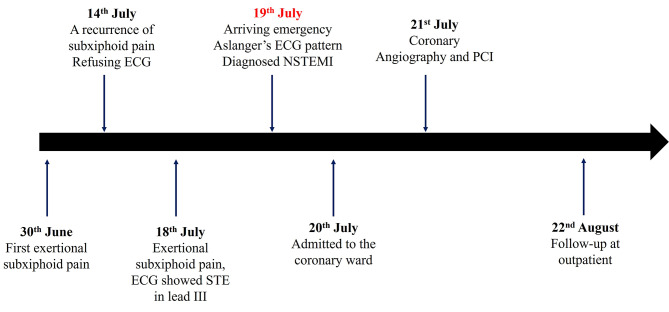
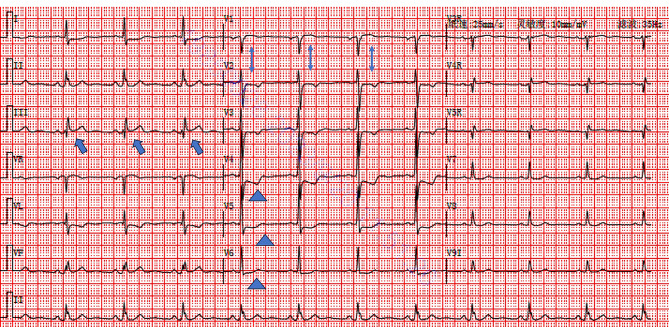
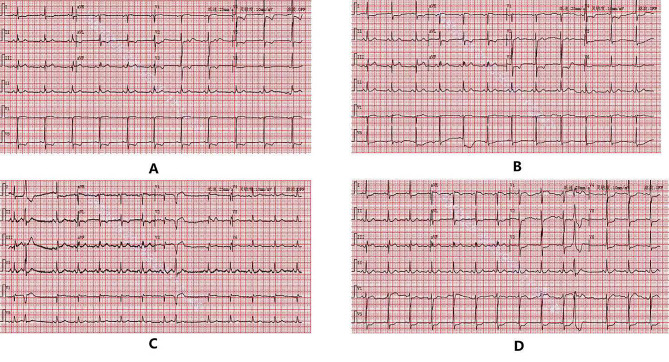
The patient was a 62-year-old male with chief complaint of intermittent exertional subxiphoid pain for 20 days from 30th June. One day after the last episode (19th July), the 18-lead electrocardiogram showed ST segment elevation of 0.05-0.1mV in lead III, ST segment depression in leads I, avL, and V2-V6, T wave inversion with positive terminal vector in lead V4-V5, and positive T wave in lead V6, which indicated Aslanger's pattern. With increased Troponin I (0.162ng/mL, 0-0.02), The patient was diagnosed as acute non-ST-segment elevation myocardial infarction (NSTEMI) and admitted to coronary ward on 20th July. The coronary angiography showed 95% stenosis in the distal left main coronary artery (LM) to the ostium of the left anterior descending artery (LAD), 90% stenosis in the proximal segment of the LAD, and 80% stenosis in the middle segment of the LAD, and TIMI blood flow was graded score 2. Three drug-eluting stents were implanted at the lesions. The patient's ECG returned close to normal one month after revascularization.
We presented an acute coronary syndrome case whose ECG showed with Aslanger's pattern (i.e., isolated ST-segment elevation in lead III, associated ST-segment depression in lead V4-V6 with positive T wave/terminal vector, and greater ST-segment elevation in lead V1 than in lead V2), and was confirmed severe stenosis of the LM and the proximal segment of the LAD via coronary angiography. In clinical practice, especially in the emergency, patients with ECG presenting Aslanger's pattern should be urgently evaluated with prompt treatment, and the timing of emergency coronary angiography and revascularization should be evaluated to avoid adverse outcomes caused by delayed treatment.
心电图(ECG)中的 Aslanger 图形表明患者可能患有急性下壁心肌梗死(AMI),同时其他冠状动脉存在临界狭窄,需要评估血运重建的时机,将其视为 ST 段抬高型心肌梗死(STEMI)的等效风险。
患者,男性,62 岁,主因间断性胸骨下劳累性疼痛 20 天,于 6 月 30 日就诊。末次发作后 1 天(7 月 19 日),18 导联心电图显示 III 导联 ST 段抬高 0.05-0.1mV,I、avL 和 V2-V6 导联 ST 段压低,V4-V5 导联 T 波倒置,正向终末向量,V6 导联 T 波正向,提示 Aslanger 图形。肌钙蛋白 I 升高(0.162ng/ml,0-0.02),诊断为急性非 ST 段抬高型心肌梗死(NSTEMI),于 7 月 20 日收入心内科病房。冠状动脉造影显示左主干(LM)远段至左前降支(LAD)开口处狭窄 95%,LAD 近段狭窄 90%,中段狭窄 80%,TIMI 血流分级 2 级。于病变处植入 3 枚药物洗脱支架。血管重建术后 1 个月,患者心电图恢复接近正常。
我们报告了 1 例急性冠状动脉综合征患者,其心电图呈 Aslanger 图形(即 III 导联孤立性 ST 段抬高,V4-V6 导联 ST 段压低伴正向 T 波/终末向量,V1 导联 ST 段抬高大于 V2 导联),经冠状动脉造影证实 LM 和 LAD 近段严重狭窄。在临床实践中,特别是在急诊情况下,出现心电图 Aslanger 图形的患者应紧急评估,及时治疗,并评估紧急冠状动脉造影和血运重建的时机,以避免因治疗延迟而导致不良后果。