Neurosurgery Unit B, Bordeaux University Hospital, Pellegrin Hospital, 33000, Bordeaux, France.
Neurological ICU, Bordeaux University Hospital, Pellegrin Hospital, 33000, Bordeaux, France.
Dysphagia. 2024 Aug;39(4):552-572. doi: 10.1007/s00455-023-10646-2. Epub 2024 Jan 8.
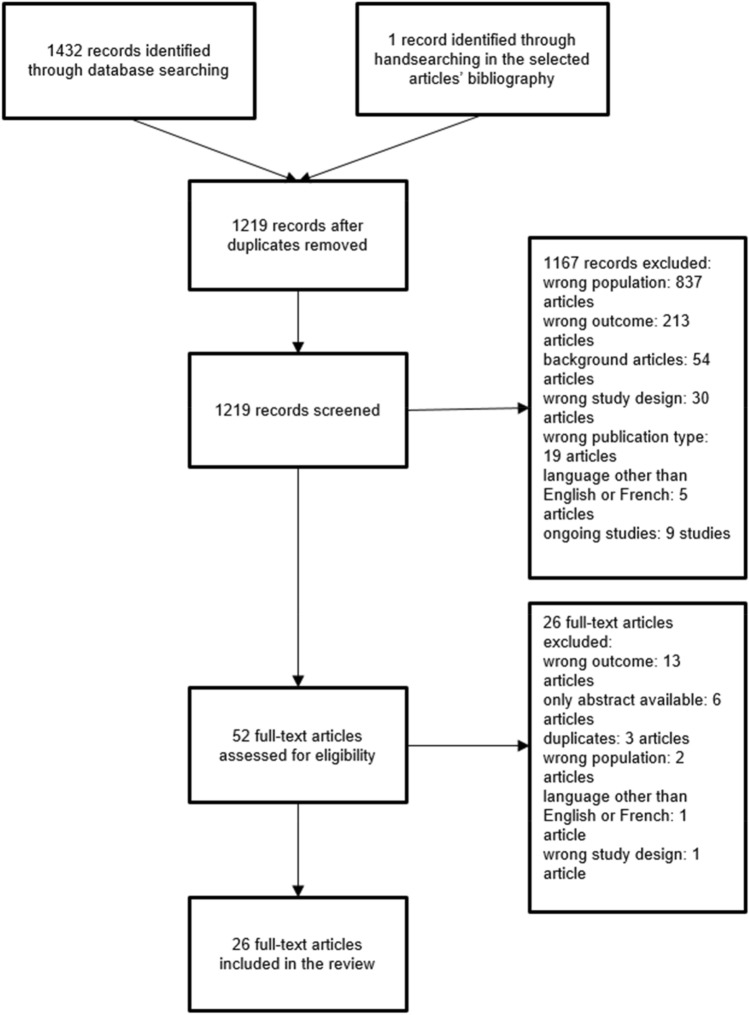
Neurological patients frequently have disorders of consciousness, swallowing disorders, or neurological states that are incompatible with extubation. Therefore, they frequently require tracheostomies during their stay in an intensive care unit. After the acute phase, tracheostomy weaning and decannulation are generally expected to promote rehabilitation. However, few reliable predictive factors (PFs) for decannulation have been identified in this patient population. We sought to identify PFs that may be used during tracheostomy weaning and decannulation in patients with brain injuries. We conducted a systematic review of the literature regarding potential PFs for decannulation; searches were performed on 16 March 2021 and 1 June 2022. The following databases were searched: MEDLINE, EMBASE, CINAHL, Scopus, Web of Science, PEDro, OPENGREY, OPENSIGLE, Science Direct, CLINICAL TRIALS and CENTRAL. We searched for all article types, except systematic reviews, meta-analyses, abstracts, and position articles. Retrieved articles were published in English or French, with no date restriction. In total, 1433 articles were identified; 26 of these were eligible for inclusion in the review. PFs for successful decannulation in patients with acquired brain injuries (ABIs) included high neurological status, traumatic brain injuries rather than stroke or anoxic brain lesions, younger age, effective swallowing, an effective cough, and the absence of pulmonary infections. Secondary PFs included early tracheostomy, supratentorial lesions, the absence of critical illness polyneuropathy/myopathy, and the absence of tracheal lesions. To our knowledge, this is the first systematic review to identify PFs for decannulation in patients with ABIs. These PFs may be used by clinicians during tracheostomy weaning.
神经疾病患者常存在意识障碍、吞咽障碍或与拔管不兼容的神经状态,因此他们在重症监护病房住院期间常需行气管切开术。在急性阶段后,气管切开术脱机和拔管通常预期可促进康复。然而,在该患者人群中,很少有可靠的拔管预测因素(PFs)被确定。我们试图确定在脑损伤患者中进行气管切开术脱机和拔管时可能使用的 PF。我们对有关拔管潜在 PF 的文献进行了系统回顾;检索于 2021 年 3 月 16 日和 2022 年 6 月 1 日进行。搜索了以下数据库:MEDLINE、EMBASE、CINAHL、Scopus、Web of Science、PEDro、OPENGREY、OPENSIGLE、Science Direct、CLINICAL TRIALS 和 CENTRAL。我们搜索了所有类型的文章,除了系统评价、荟萃分析、摘要和立场文章。检索到的文章以英文或法文发表,无日期限制。共确定了 1433 篇文章,其中 26 篇文章符合纳入审查的条件。脑外伤后(ABI)患者成功拔管的 PF 包括高神经状态、创伤性脑损伤而非中风或缺氧性脑损伤、年龄较小、有效吞咽、有效咳嗽以及无肺部感染。次要 PF 包括早期气管切开术、幕上病变、无危重病多发性神经病/肌病以及无气管损伤。据我们所知,这是首次系统评价确定 ABI 患者拔管的 PF。这些 PF 可在气管切开术脱机期间由临床医生使用。