Department of Human Anatomy and Medical Physiology, University of Nairobi, P.O. Box 30197, Nairobi, 00100, Kenya.
University Hospital Wuerzburg, Clinic and Policlinic for Psychiatry, Psychosomatics and Psychotherapy Margarete-Höppel-Platz 1, 97080, Würzburg, Germany.
J Neural Transm (Vienna). 2024 Dec;131(12):1429-1453. doi: 10.1007/s00702-023-02723-5. Epub 2024 Jan 23.
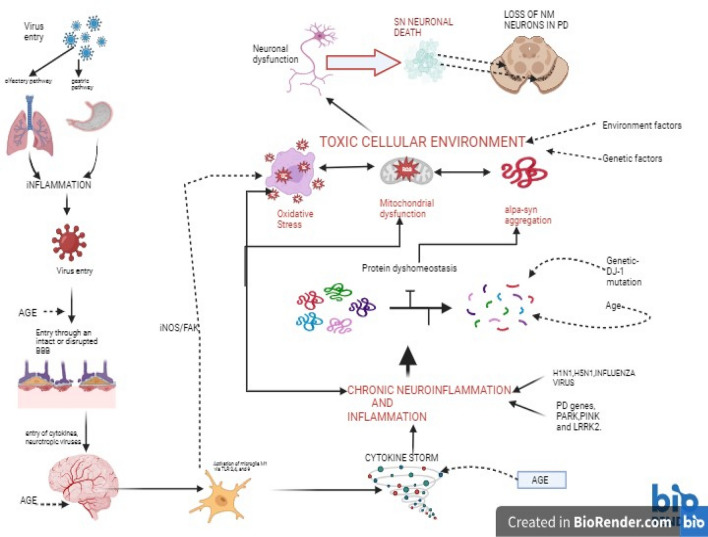
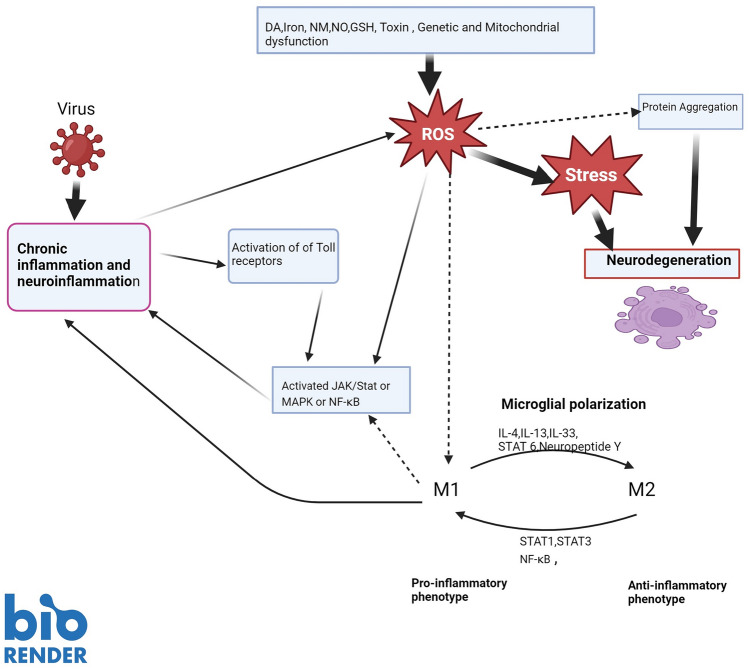
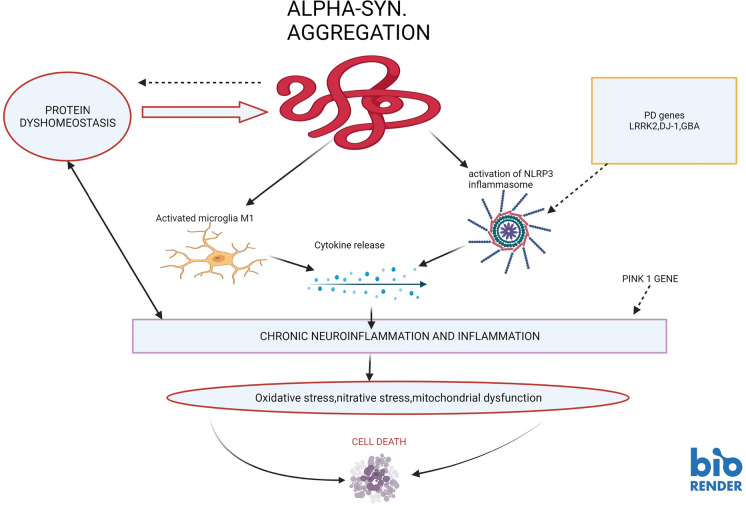
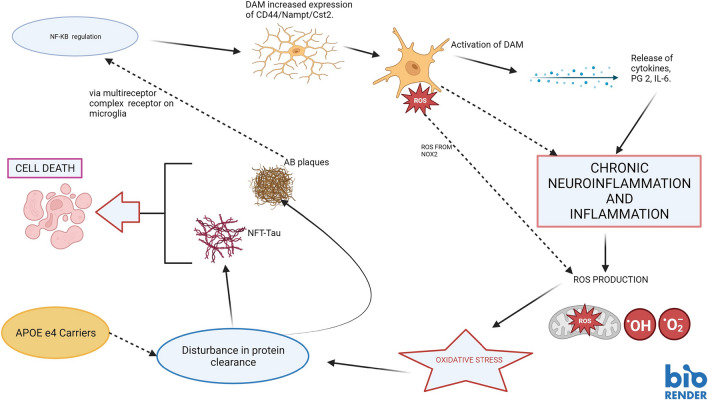
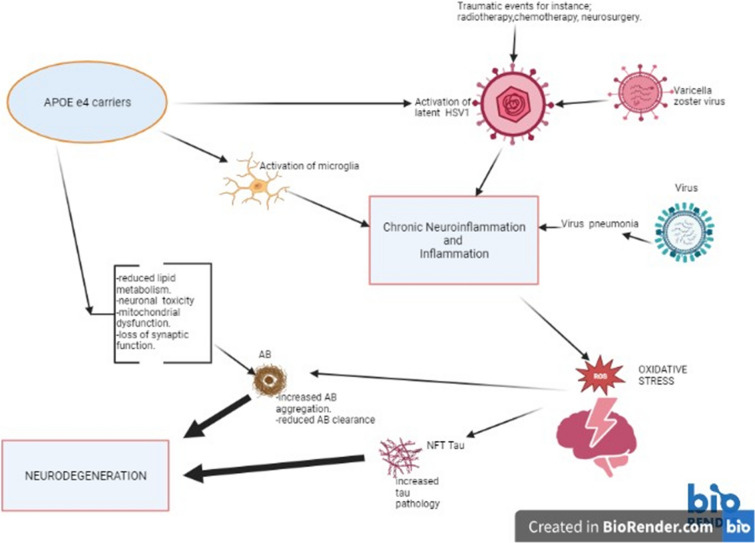
Fascinatingly, an abundance of recent studies has subscribed to the importance of cytotoxic immune mechanisms that appear to increase the risk/trigger for many progressive neurodegenerative disorders, including Parkinson's disease (PD), Alzheimer's disease (AD), amyotrophic lateral sclerosis, and multiple sclerosis. Events associated with the neuroinflammatory cascades, such as ageing, immunologic dysfunction, and eventually disruption of the blood-brain barrier and the "cytokine storm", appear to be orchestrated mainly through the activation of microglial cells and communication with the neurons. The inflammatory processes prompt cellular protein dyshomeostasis. Parkinson's and Alzheimer's disease share a common feature marked by characteristic pathological hallmarks of abnormal neuronal protein accumulation. These Lewy bodies contain misfolded α-synuclein aggregates in PD or in the case of AD, they are Aβ deposits and tau-containing neurofibrillary tangles. Subsequently, these abnormal protein aggregates further elicit neurotoxic processes and events which contribute to the onset of neurodegeneration and to its progression including aggravation of neuroinflammation. However, there is a caveat for exclusively linking neuroinflammation with neurodegeneration, since it's highly unlikely that immune dysregulation is the only factor that contributes to the manifestation of many of these neurodegenerative disorders. It is unquestionably a complex interaction with other factors such as genetics, age, and environment. This endorses the "multiple hit hypothesis". Consequently, if the host has a genetic susceptibility coupled to an age-related weakened immune system, this makes them more susceptible to the virus/bacteria-related infection. This may trigger the onset of chronic cytotoxic neuroinflammatory processes leading to protein dyshomeostasis and accumulation, and finally, these events lead to neuronal destruction. Here, we differentiate "neuroinflammation" and "inflammation" with regard to the involvement of the blood-brain barrier, which seems to be intact in the case of neuroinflammation but defect in the case of inflammation. There is a neuroinflammation-inflammation continuum with regard to virus-induced brain affection. Therefore, we propose a staging of this process, which might be further developed by adding blood- and CSF parameters, their stage-dependent composition and stage-dependent severeness grade. If so, this might be suitable to optimise therapeutic strategies to fight brain neuroinflammation in its beginning and avoid inflammation at all.
有趣的是,大量最近的研究都认为细胞毒性免疫机制很重要,这些机制似乎会增加许多进行性神经退行性疾病的风险/触发因素,包括帕金森病(PD)、阿尔茨海默病(AD)、肌萎缩侧索硬化症和多发性硬化症。与神经炎症级联相关的事件,如衰老、免疫功能障碍,最终破坏血脑屏障和“细胞因子风暴”,似乎主要通过小胶质细胞的激活和与神经元的通信来协调。炎症过程促使细胞蛋白的动态平衡失调。帕金森病和阿尔茨海默病有一个共同的特征,即神经元蛋白异常积累的特征性病理标志。这些路易体包含 PD 中的错误折叠的α-突触核蛋白聚集物,或者在 AD 的情况下,它们是 Aβ沉积物和含有 tau 的神经原纤维缠结。随后,这些异常蛋白聚集体进一步引发神经毒性过程和事件,导致神经退行性变的发生和进展,包括神经炎症的加重。然而,将神经炎症与神经退行性变完全联系起来有一个警告,因为免疫失调不太可能是导致许多神经退行性疾病表现的唯一因素。毫无疑问,这是与其他因素(如遗传、年龄和环境)的复杂相互作用。这支持了“多重打击假说”。因此,如果宿主有遗传易感性,加上与年龄相关的免疫系统减弱,这会使他们更容易受到与病毒/细菌相关的感染。这可能会引发慢性细胞毒性神经炎症过程,导致蛋白动态平衡失调和积累,最终导致神经元破坏。在这里,我们区分了“神经炎症”和“炎症”,涉及血脑屏障的参与,在神经炎症的情况下,血脑屏障似乎是完整的,但在炎症的情况下,血脑屏障是有缺陷的。在病毒引起的脑损伤方面,存在神经炎症-炎症连续体。因此,我们提出了这个过程的分期,通过添加血液和 CSF 参数及其与分期相关的组成和分期相关的严重程度等级,这个分期可能会进一步发展。如果是这样,这可能适合优化治疗策略,以在开始时对抗大脑神经炎症,并避免炎症的发生。