Schmutzer-Sondergeld Michael, Gencer Aylin, Niedermeyer Sebastian, Quach Stefanie, Stoecklein Veit M, Teske Nico, Schichor Christian, Terpolilli Nicole Angela, Kunz Mathias, Thon Niklas
Department of Neurosurgery, LMU University Hospital, LMU Munich, Marchioninistrasse 15, 81377, Munich, Germany.
Acta Neurochir (Wien). 2024 Jan 27;166(1):39. doi: 10.1007/s00701-024-05950-1.
The best treatment strategies for cerebral arachnoid cysts (CAC) are still up for debate. In this study, we present CAC management, outcome data, and risk factors for recurrence after surgical treatment, focusing on microscopic/endoscopic approaches as compared to minimally invasive stereotactic procedures in children and adults.
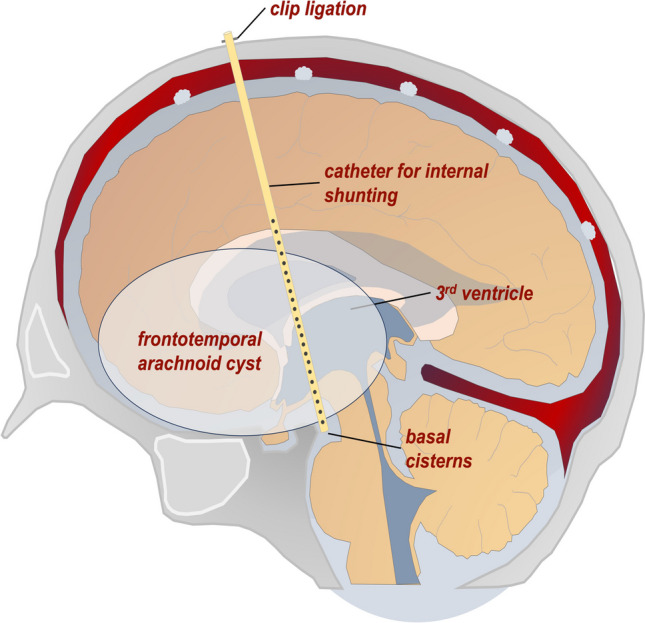
In our single-institution retrospective database, we identified all patients treated surgically for newly diagnosed CAC between 2000 and 2022. Microscopic/endoscopic surgery (ME) aimed for safe cyst wall fenestration. Stereotactic implantation of an internal shunt catheter (STX) to drain CAC into the ventricles and/or cisterns was used as an alternative procedure in patients aged ≥ 3 years. Treatment decisions in favor of ME vs. STX were made by interdisciplinary consensus. The primary study endpoint was time to CAC recurrence (TTR). Secondary endpoints were outcome metrics including clinical symptoms and MR-morphological analyses. Data analysis included subdivision of the total cohort into three distinct age groups (AG1, < 6 years; AG2, 6-18 years; AG3, ≥ 18 years).
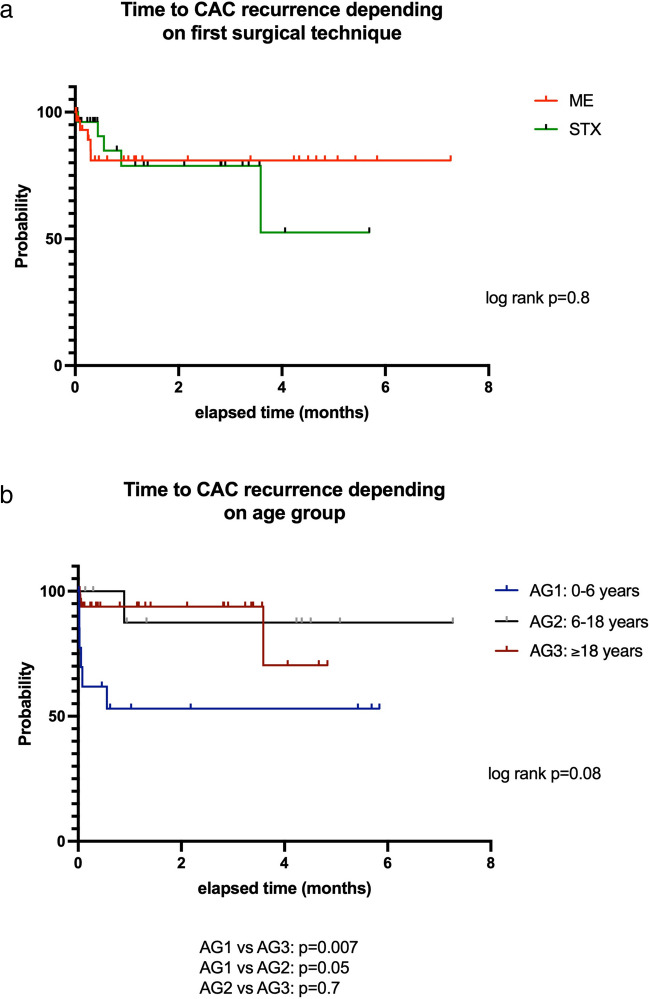
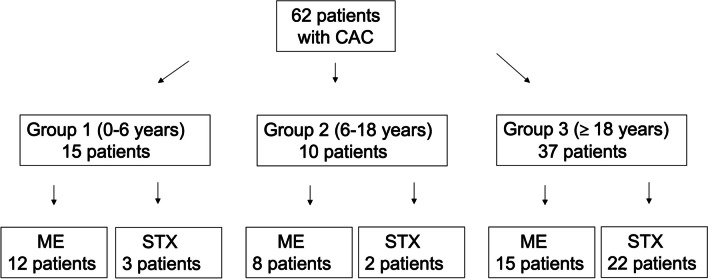
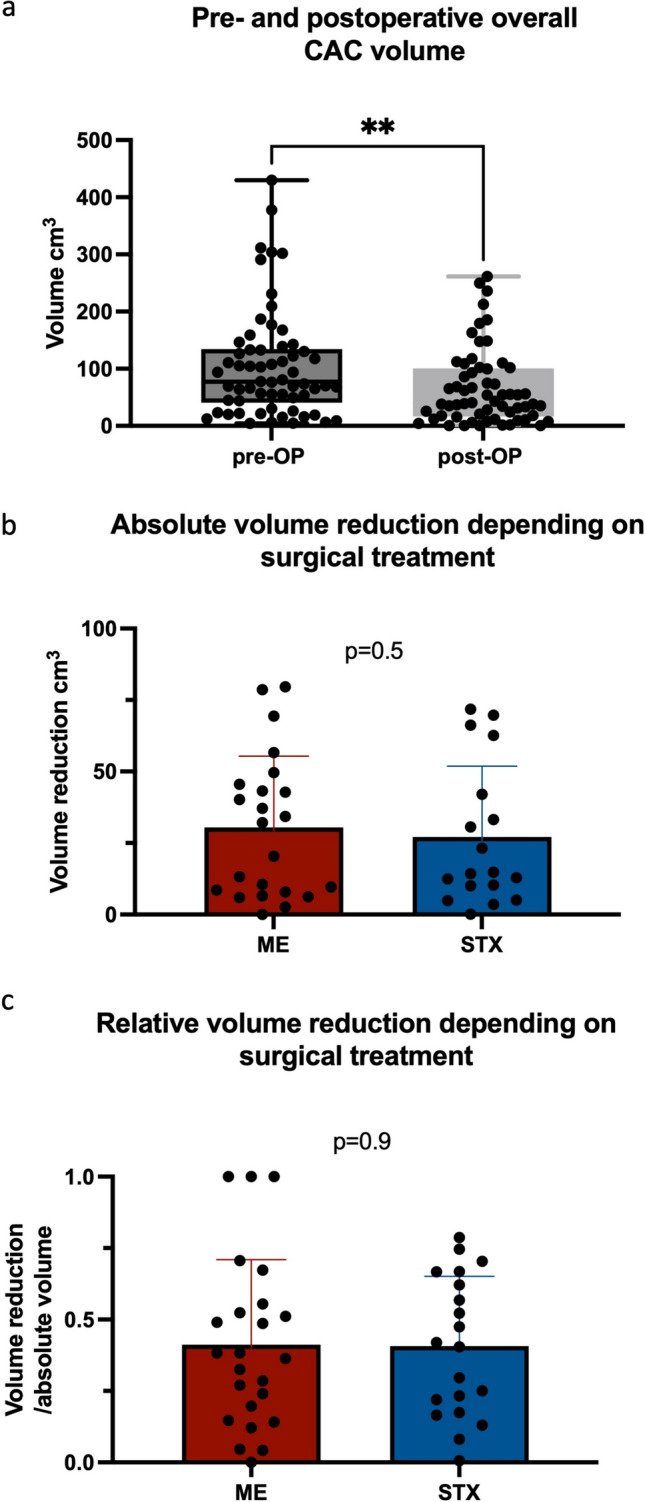
Sixty-two patients (median age 26.5 years, range 0-82 years) were analyzed. AG1 included 15, AG2 10, and AG3 37 patients, respectively. The main presenting symptoms were headache and vertigo. In AG1 hygromas, an increase in head circumference and thinning of cranial calvaria were most frequent. Thirty-five patients underwent ME and 27 STX, respectively; frequency did not differ between AGs. There were two (22.2%) periprocedural venous complications in infants (4- and 10-month-old) during an attempt at prepontine fenestration of a complex CAC, one with fatal outcome in a 10-month-old boy. Other complications included postoperative bleeding (2, 22.2%), CSF leaks (4, 44.4%), and meningitis (1, 11.1%). Overall, clinical improvement and significant volume reduction (p = 0.008) were seen in all other patients; this did not differ between AGs. Median follow-up for all patients was 25.4 months (range, 3.1-87.1 months). Recurrent cysts were seen in 16.1%, independent of surgical procedure used (p = 0.7). In cases of recurrence, TTR was 7.9 ± 12.7 months. Preoperative ventricular expansion (p = 0.03), paresis (p = 0.008), and age under 6 years (p = 0.03) were significant risk factors for CAC recurrence in multivariate analysis.
In patients suffering from CAC, both ME and STX can improve clinical symptoms at low procedural risk, with equal extent of CAC volume reduction. However, in infants and young children, CAC are more often associated with severe clinical symptoms, stereotactic procedures have limited use, and microsurgery in the posterior fossa may bear the risk of severe venous bleeding.
脑蛛网膜囊肿(CAC)的最佳治疗策略仍存在争议。在本研究中,我们介绍了CAC的治疗方法、预后数据以及手术治疗后复发的危险因素,重点关注与儿童和成人微创立体定向手术相比的显微镜/内镜手术方法。
在我们的单机构回顾性数据库中,我们确定了2000年至2022年间所有因新诊断的CAC接受手术治疗的患者。显微镜/内镜手术(ME)旨在安全地进行囊肿壁开窗。对于年龄≥3岁的患者,采用立体定向植入内分流导管(STX)将CAC引流至脑室和/或脑池作为替代手术。支持ME与STX的治疗决策通过多学科共识做出。主要研究终点是CAC复发时间(TTR)。次要终点是包括临床症状和磁共振形态学分析在内的预后指标。数据分析包括将整个队列细分为三个不同的年龄组(AG1,<6岁;AG2,6 - 18岁;AG3,≥18岁)。
分析了62例患者(中位年龄26.5岁,范围0 - 82岁)。AG1组有15例,AG2组有10例,AG3组有37例。主要表现症状为头痛和眩晕。在AG1组的蛛网膜下腔积水病例中,头围增加和颅骨变薄最为常见。分别有35例患者接受了ME手术和27例患者接受了STX手术;各年龄组之间的频率无差异。在试图对复杂的CAC进行脑桥前开窗时,两名婴儿(4个月和10个月大)出现了围手术期静脉并发症(22.2%),其中一名10个月大男孩死亡。其他并发症包括术后出血(2例,22.2%)、脑脊液漏(4例,44.4%)和脑膜炎(1例,11.1%)。总体而言,所有其他患者均有临床改善和囊肿体积显著减小(p = 0.008);各年龄组之间无差异。所有患者的中位随访时间为25.4个月(范围,3.1 - 87.1个月)。16.1%的患者出现复发性囊肿,与所采用的手术方法无关(p = 0.7)。在复发病例中,TTR为7.9±12.7个月。多因素分析显示,术前脑室扩张(p = 0.03)、轻瘫(p = 0.008)和6岁以下年龄(p = 0.03)是CAC复发的显著危险因素。
对于患有CAC的患者,ME和STX均可在低手术风险下改善临床症状,且囊肿体积减小程度相同。然而,在婴幼儿中,CAC更常与严重临床症状相关,立体定向手术应用有限,而后颅窝显微手术可能存在严重静脉出血风险。