Department of Surgery, Örebro University and University Hospital, Örebro, Sweden.
University Centre for Vascular Medicine and Department of Medicine-Section Angiology, University Hospital Carl Gustav Carus at the Technische Universität Dresden, Dresden, Germany.
Br J Surg. 2024 Jan 31;111(2). doi: 10.1093/bjs/znad437.
Revascularization is the primary treatment modality for chronic limb-threatening ischaemia (CLTI), but is not feasible in all patients. PLX-PAD is an off-the-shelf, placental-derived, mesenchymal stromal cell-like cell therapy. This study aimed to evaluate whether PLX-PAD would increase amputation-free survival in people with CLTI who were not candidates for revascularization.
People with CLTI and minor tissue loss (Rutherford 5) who were unsuitable for revascularization were entered into a randomized, parallel-group, placebo-controlled, multinational, blinded, trial, in which PLX-PAD was compared with placebo (2 : 1 randomization), with 30 intramuscular injections (0.5 ml each) into the index leg on days 0 and 60. Planned follow-up was 12-36 months, and included vital status, amputations, lesion size, pain and quality-of-life assessments, haemodynamic parameters, and adverse events.
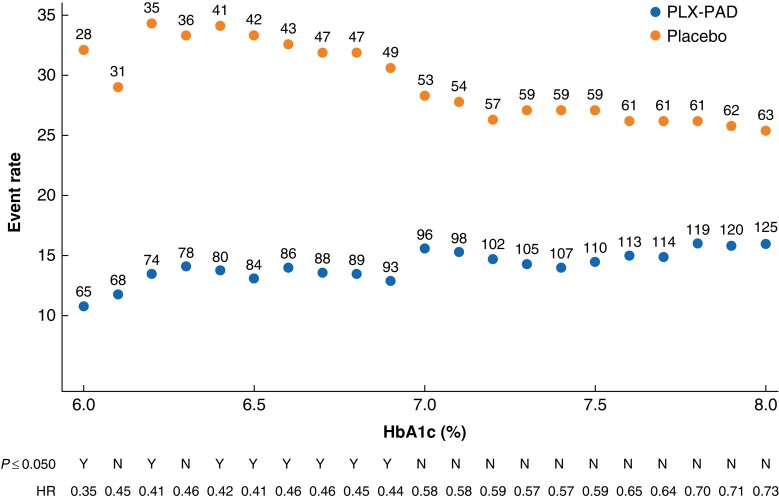
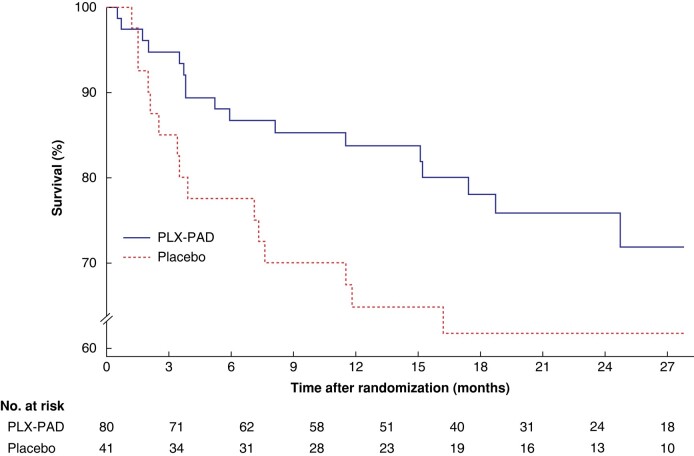
Of 213 patients enrolled, 143 were randomized to PLX-PAD and 70 to placebo. Demographics and baseline characteristics were balanced. Most patients were Caucasian (96.2%), male (76.1%), and ambulatory (85.9%). Most patients (76.6%) reported at least one adverse event, which were mostly expected events in CLTI, such as skin ulcer or gangrene. The probability of major amputation or death was similar for placebo and PLX-PAD (33 and 28.6% respectively; HR 0.93, 95% c.i. 0.53 to 1.63; P = 0.788). Revascularization and complete wound healing rates were similar in the two groups. A post hoc analysis of a subpopulation of 121 patients with a baseline haemoglobin A1c level below 6.5% showed improved 12-month amputation-free survival (HR 0.46, 0.21 to 0.99; P = 0.048).
Although there was no evidence that PLX-PAD reduced amputation-free survival in the entire study population, benefit was observed in patients without diabetes mellitus or whose diabetes was well controlled; this requires confirmation in further studies. Trial registration: NCT03006770 (http://www.clinicaltrials.gov); 2015-005532-18 (EudraCT Clinical Trials register - Search for 2015-005532-18).
血运重建是治疗慢性肢体严重缺血(CLTI)的主要方法,但并非所有患者都适用。PLX-PAD 是一种现成的、胎盘来源的、间充质基质细胞样细胞疗法。本研究旨在评估 PLX-PAD 是否会增加不适合血运重建的 CLTI 患者的无截肢生存率。
纳入 CLTI 伴小组织损失(Rutherford 5)且不适合血运重建的患者,进行一项随机、平行组、安慰剂对照、多国、盲法、试验,将 PLX-PAD 与安慰剂(2:1 随机化)进行比较,30 名患者在第 0 天和第 60 天接受 30 次肌肉内注射(每次 0.5ml)至索引腿。计划的随访时间为 12-36 个月,包括生命状态、截肢、病变大小、疼痛和生活质量评估、血流动力学参数和不良事件。
在纳入的 213 名患者中,143 名被随机分配至 PLX-PAD 组,70 名被分配至安慰剂组。两组患者的人口统计学和基线特征均衡。大多数患者为白种人(96.2%)、男性(76.1%)和有活动能力的(85.9%)。大多数患者(76.6%)报告至少有一次不良事件,这些事件大多是 CLTI 中预期的事件,如皮肤溃疡或坏疽。安慰剂组和 PLX-PAD 组的主要截肢或死亡概率相似(分别为 33%和 28.6%;HR 0.93,95%CI 0.53 至 1.63;P = 0.788)。两组的血运重建和完全伤口愈合率相似。对基线糖化血红蛋白水平低于 6.5%的 121 名患者的亚组进行事后分析显示,12 个月无截肢生存率有所提高(HR 0.46,0.21 至 0.99;P = 0.048)。
尽管没有证据表明 PLX-PAD 降低了整个研究人群的无截肢生存率,但在没有糖尿病或糖尿病控制良好的患者中观察到了益处;这需要进一步研究证实。试验注册:NCT03006770(http://www.clinicaltrials.gov);2015-005532-18(EudraCT 临床试验注册-搜索 2015-005532-18)。