Medical Thoracic Oncology Unit, IRCCS Istituto Tumori "Giovanni Paolo II", Bari, Italy.
Department of Precision Medicine, University of Campania Luigi Vanvitelli, Naples, Italy.
Front Immunol. 2024 Jan 18;14:1289434. doi: 10.3389/fimmu.2023.1289434. eCollection 2023.
Consolidative thoracic radiotherapy (TRT) has been commonly used in the management of extensive-stage small cell lung cancer (ES-SCLC). Nevertheless, phase III trials exploring first-line chemoimmunotherapy have excluded this treatment approach. However, there is a strong biological rationale to support the use of radiotherapy (RT) as a boost to sustain anti-tumor immune responses. Currently, the benefit of TRT after chemoimmunotherapy remains unclear. The present report describes the real-world experiences of 120 patients with ES-SCLC treated with different chemoimmunotherapy combinations. Preclinical data supporting the hypothesis of anti-tumor immune responses induced by RT are also presented.
A total of 120 ES-SCLC patients treated with chemoimmunotherapy since 2019 in the South of Italy were retrospectively analyzed. None of the patients included in the analysis experienced disease progression after undergoing first-line chemoimmunotherapy. Of these, 59 patients underwent TRT after a multidisciplinary decision by the treatment team. Patient characteristics, chemoimmunotherapy schedule, and timing of TRT onset were assessed. Safety served as the primary endpoint, while efficacy measured in terms of overall survival (OS) and progression-free survival (PFS) was used as the secondary endpoint. Immune pathway activation induced by RT in SCLC cells was explored to investigate the biological rationale for combining RT and immunotherapy.
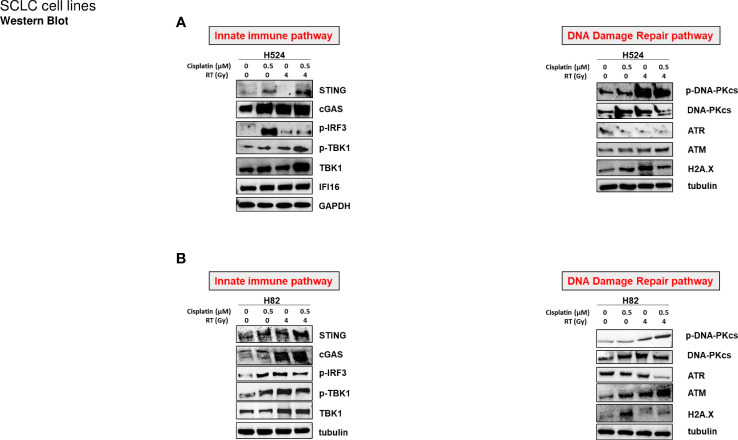
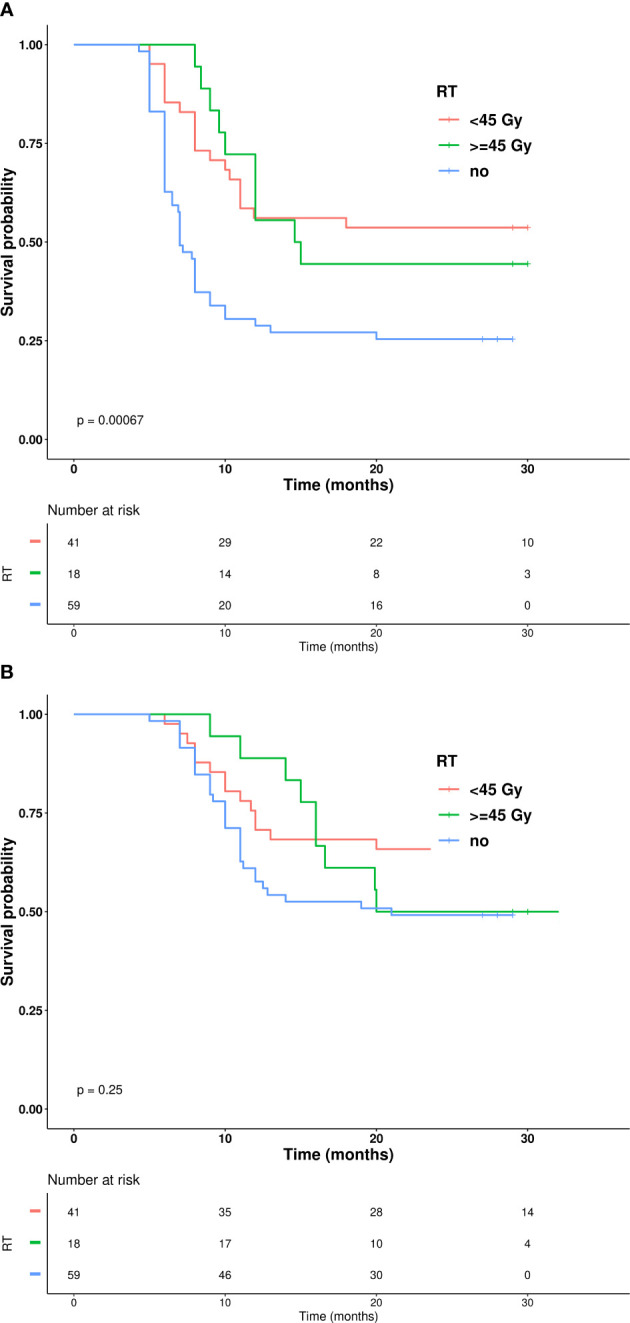
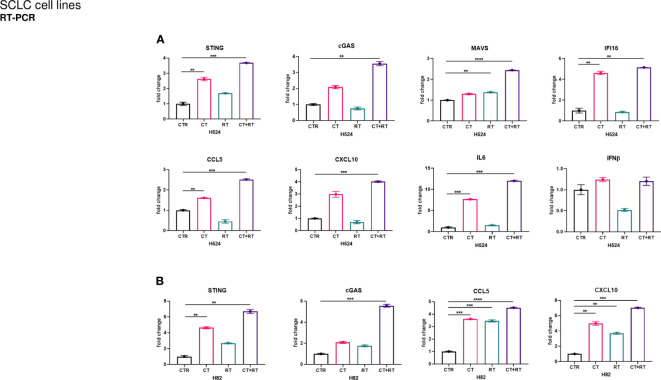
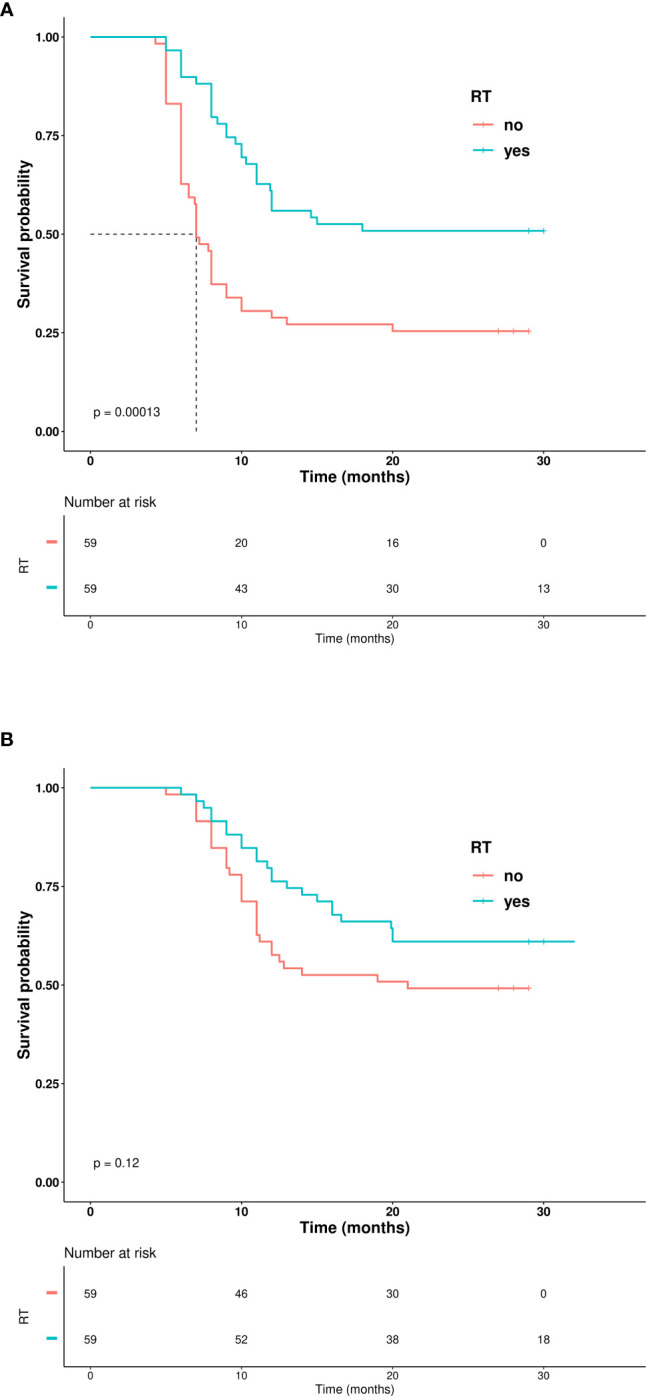
Preclinical data supported the activation of innate immune pathways, including the STimulator of INterferon pathway (STING), gamma-interferon-inducible protein (IFI-16), and mitochondrial antiviral-signaling protein (MAVS) related to DNA and RNA release. Clinical data showed that TRT was associated with a good safety profile. Of the 59 patients treated with TRT, only 10% experienced radiation toxicity, while no ≥ G3 radiation-induced adverse events occurred. The median time for TRT onset after cycles of chemoimmunotherapy was 62 days. Total radiation dose and fraction dose of TRT include from 30 Gy in 10 fractions, up to definitive dose in selected patients. Consolidative TRT was associated with a significantly longer PFS than systemic therapy alone (one-year PFS of 61% vs. 31%, p<0.001), with a trend toward improved OS (one-year OS of 80% vs. 61%, p=0.027).
Multi-center data from establishments in the South of Italy provide a general confidence in using TRT as a consolidative strategy after chemoimmunotherapy. Considering the limits of a restrospective analysis, these preliminary results support the feasibility of the approach and encourage a prospective evaluation.
巩固性胸部放疗(TRT)常用于广泛期小细胞肺癌(ES-SCLC)的治疗。然而,探索一线化疗免疫治疗的 III 期试验排除了这种治疗方法。然而,有强有力的生物学依据支持将放疗(RT)作为维持抗肿瘤免疫反应的辅助治疗。目前,化疗免疫治疗后 TRT 的获益尚不清楚。本报告描述了意大利南部 120 例接受不同化疗免疫治疗组合治疗的 ES-SCLC 患者的真实世界经验。还介绍了支持 RT 诱导抗肿瘤免疫反应的临床前数据。
回顾性分析了自 2019 年以来在意大利南部接受化疗免疫治疗的 120 例 ES-SCLC 患者。纳入分析的患者均未在接受一线化疗免疫治疗后发生疾病进展。其中,59 例患者经治疗团队多学科决策后接受 TRT。评估了患者特征、化疗免疫治疗方案和 TRT 开始时间。安全性为主要终点,总生存期(OS)和无进展生存期(PFS)作为次要终点评估疗效。探索 RT 诱导 SCLC 细胞中免疫途径激活的作用,以研究将 RT 与免疫治疗相结合的生物学依据。
临床前数据支持固有免疫途径的激活,包括 STimulator of INterferon 途径(STING)、γ干扰素诱导蛋白(IFI-16)和与 DNA 和 RNA 释放相关的线粒体抗病毒信号蛋白(MAVS)。临床数据显示,TRT 安全性良好。59 例接受 TRT 治疗的患者中,仅 10%发生放射性毒性,无≥G3 级放射性不良反应发生。TRT 开始时间距化疗免疫治疗周期中位时间为 62 天。TRT 的总辐射剂量和分次剂量包括 30Gy/10 次,在选定患者中可采用根治性剂量。巩固性 TRT 与单纯系统治疗相比,PFS 显著延长(一年 PFS 为 61% vs. 31%,p<0.001),OS 有改善趋势(一年 OS 为 80% vs. 61%,p=0.027)。
来自意大利南部机构的多中心数据为在化疗免疫治疗后将 TRT 作为巩固性策略的使用提供了普遍信心。考虑到回顾性分析的局限性,这些初步结果支持该方法的可行性,并鼓励进行前瞻性评估。