Department of Cardiology and Angiology, University Heart Center Freiburg - Bad Krozingen, Faculty of Medicine, University of Freiburg, Freiburg, Germany.
Department of Cardiology, Angiology, Haemostaseology and Medical Intensive Care, Medical Center Mannheim, Medical Faculty Mannheim, Heidelberg University, Heidelberg, Germany.
J Thromb Thrombolysis. 2024 Mar;57(3):361-369. doi: 10.1007/s11239-023-02937-0. Epub 2024 Feb 12.
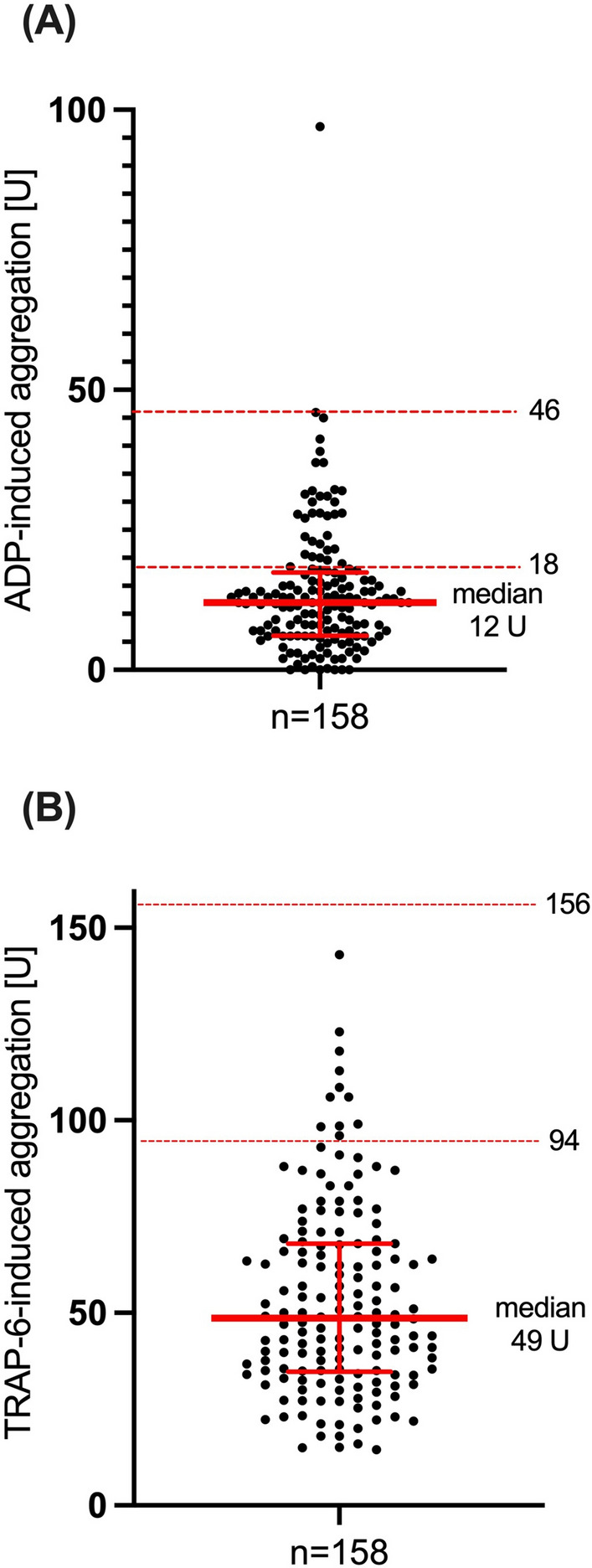
High on-clopidogrel platelet reactivity (HPR) associates with ischemic risk in patients after percutaneous intervention (PCI). This study aimed to evaluate the association of HPR as assessed by multiple electrode aggregometry (MEA) with ischemic, thromboembolic, and bleeding risk in patients with atrial fibrillation (AF) undergoing PCI. Patients with AF and an indication for oral anticoagulation (OAC) were included in this prospective cohort study on day 1-3 after PCI. Platelet aggregation [U] was analyzed by MEA. HPR and low platelet reactivity (LPR) were defined as ADP-induced aggregation ≥ 46 U and ≤ 18 U, respectively. TRAP-6-induced aggregation reference was 94-156 U. The primary outcome was time to all-cause death, myocardial infarction, or stroke at 6 months. The secondary outcome was time to non-major clinically relevant bleedings or major bleedings. 159 patients were enrolled between May 2020 and May 2021. The median age was 78 years (interquartile range 72-82) and 111 (70%) were male. Median ADP- and TRAP-induced aggregation were 12 (6-17) and 49 (35-68) U, respectively. 147 (93%) patients had a low overall aggregability. HPR was detected in 2 patients (1%) and 125 (79%) had LPR. ADP-induced aggregation did not significantly associate with the primary outcome (r = 0.081, p = 0.309) but correlated inversely with bleeding risk (r = - 0.201, p = 0.011). HPR status as assessed by MEA among patients with AF after PCI was rare and overall aggregability was low. Conventional cut-off values for HPR might be inappropriate for these patients. ADP-induced aggregation might be helpful to identify patients at risk for bleeding.
高氯吡格雷血小板反应性(HPR)与经皮介入治疗(PCI)后的患者缺血风险相关。本研究旨在评估经多电极聚集仪(MEA)评估的 HPR 与接受 PCI 的房颤(AF)患者的缺血、血栓栓塞和出血风险之间的相关性。该前瞻性队列研究纳入了 PCI 后第 1-3 天有口服抗凝治疗(OAC)指征的 AF 患者。通过 MEA 分析血小板聚集[U]。HPR 和低血小板反应性(LPR)定义为 ADP 诱导的聚集≥46 U 和≤18 U。TRAP-6 诱导的聚集参考值为 94-156 U。主要终点为 6 个月时全因死亡、心肌梗死或卒中的时间。次要终点为非主要临床相关出血或大出血的时间。2020 年 5 月至 2021 年 5 月期间共纳入 159 例患者。中位年龄为 78 岁(四分位距 72-82),111 例(70%)为男性。中位 ADP 和 TRAP 诱导的聚集分别为 12(6-17)和 49(35-68)U。147 例(93%)患者整体聚集性较低。2 例(1%)患者存在 HPR,125 例(79%)患者存在 LPR。ADP 诱导的聚集与主要结局无显著相关性(r=0.081,p=0.309),但与出血风险呈负相关(r=-0.201,p=0.011)。在接受 PCI 的 AF 患者中,MEA 评估的 HPR 状态罕见,整体聚集性较低。对于这些患者,HPR 的常规截断值可能不合适。ADP 诱导的聚集可能有助于识别出血风险患者。