Field Epidemiology Training Program, Infectious Diseases Surveillance Center, National Institute of Infectious Diseases, Tokyo, Japan.
Center for Field Epidemic Intelligence, Research, and Professional Development, National Institute of Infectious Diseases, Tokyo, Japan.
BMC Infect Dis. 2024 Feb 15;24(1):209. doi: 10.1186/s12879-024-09107-4.
In Japan, carbapenem-resistant Enterobacterales (CRE) infections were incorporated into the National Epidemiological Surveillance of Infectious Diseases (NESID) in 2014, necessitating mandatory reporting of all CRE infections cases. Subsequently, pathogen surveillance was initiated in 2017, which involved the collection and analysis of CRE isolates from reported cases to assess carbapenemase gene possession. In this surveillance, CRE is defined as (i) minimum inhibitory concentration (MIC) of meropenem ≥2 mg/L (MEPM criteria) or (ii) MIC of imipenem ≥2 mg/L and MIC of cefmetazole ≥64 mg/L (IPM criteria). This study examined whether the current definition of CRE surveillance captures cases with a clinical and public health burden.
CRE isolates from reported cases were collected from the public health laboratories of local governments, which are responsible for pathogen surveillance. Antimicrobial susceptibility tests were conducted on these isolates to assess compliance with the NESID CRE definition. The NESID data between April 2017 and March 2018 were obtained and analyzed using antimicrobial susceptibility test results.
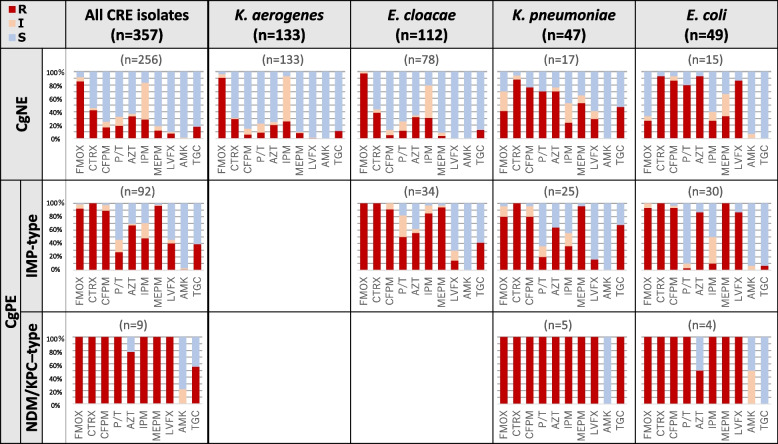
In total, 1681 CRE cases were identified during the study period, and pathogen surveillance data were available for 740 (44.0%) cases. Klebsiella aerogenes and Enterobacter cloacae complex were the dominant species, followed by Klebsiella pneumoniae and Escherichia coli. The rate of carbapenemase gene positivity was 26.5% (196/740), and 93.4% (183/196) of these isolates were of the IMP type. Meanwhile, 315 isolates were subjected to antimicrobial susceptibility testing. Among them, 169 (53.7%) fulfilled only the IPM criteria (IPM criteria-only group) which were susceptible to meropenem, while 146 (46.3%) fulfilled the MEPM criteria (MEPM criteria group). The IPM criteria-only group and MEPM criteria group significantly differed in terms of carbapenemase gene positivity (0% vs. 67.8%), multidrug resistance rates (1.2% vs. 65.8%), and mortality rates (1.8% vs 6.9%).
The identification of CRE cases based solely on imipenem resistance has had a limited impact on clinical management. Emphasizing resistance to meropenem is crucial in defining CRE, which pose both clinical and public health burden. This emphasis will enable the efficient allocation of limited health and public health resources and preservation of newly developed antimicrobials.
在日本,耐碳青霉烯肠杆菌科(CRE)感染于 2014 年被纳入国家传染病流行监测(NESID),所有 CRE 感染病例都需要强制报告。随后,于 2017 年开始进行病原体监测,包括收集和分析报告病例中的 CRE 分离株,以评估碳青霉烯酶基因的存在。在这项监测中,CRE 被定义为(i)美罗培南的最低抑菌浓度(MIC)≥2mg/L(MEPM 标准)或(ii)亚胺培南的 MIC≥2mg/L 且头孢美唑的 MIC≥64mg/L(IPM 标准)。本研究旨在评估当前的 CRE 监测定义是否能够捕捉到具有临床和公共卫生负担的病例。
从负责病原体监测的地方政府公共卫生实验室收集报告病例中的 CRE 分离株。对这些分离株进行药敏试验,以评估其是否符合 NESID CRE 定义。使用药敏试验结果对 2017 年 4 月至 2018 年 3 月期间的 NESID 数据进行了分析。
在研究期间共发现 1681 例 CRE 病例,其中 740 例(44.0%)有病原监测数据。产气肠杆菌和阴沟肠杆菌复合体是主要的菌种,其次是肺炎克雷伯菌和大肠埃希菌。碳青霉烯酶基因阳性率为 26.5%(196/740),其中 93.4%(183/196)为 IMP 型。同时,对 315 株分离株进行了药敏试验。其中,169 株(53.7%)仅符合 IPM 标准(仅 IPM 标准组),对美罗培南敏感,而 146 株(46.3%)符合 MEPM 标准(MEPM 标准组)。仅 IPM 标准组和 MEPM 标准组在碳青霉烯酶基因阳性率(0% vs. 67.8%)、多药耐药率(1.2% vs. 65.8%)和死亡率(1.8% vs. 6.9%)方面存在显著差异。
仅基于亚胺培南耐药来鉴定 CRE 病例对临床管理的影响有限。强调对美罗培南的耐药性在定义 CRE 方面至关重要,因为 CRE 具有临床和公共卫生负担。这一重点将使有限的卫生和公共卫生资源得到有效分配,并保护新开发的抗菌药物。