Department of Hematology, Radboud University Medical Center, PO Box 9101, 6500 HB, Nijmegen, The Netherlands.
Hemophilia Treatment Center, Nijmegen-Eindhoven-Maastricht, The Netherlands.
Eur J Drug Metab Pharmacokinet. 2024 Mar;49(2):191-205. doi: 10.1007/s13318-024-00876-6. Epub 2024 Feb 17.
Hemophilia A patients are treated with factor (F) VIII prophylactically to prevent bleeding. In general, dosage and frequency are based on pharmacokinetic measurements. Ideally, an alternative dose adjustment can be based on the hemostatic potential, measured with a thrombin generation assay (TGA), like the Nijmegen hemostasis assay.
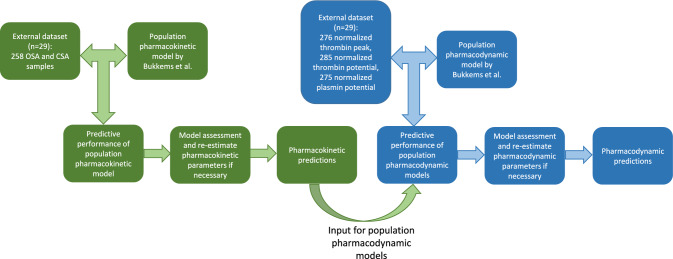
The objective of this study was to investigate the predicted performance of a previously developed pharmacokinetic-pharmacodynamic model for FVIII replacement therapy, relating FVIII dose and FVIII activity levels with thrombin and plasmin generation parameters.
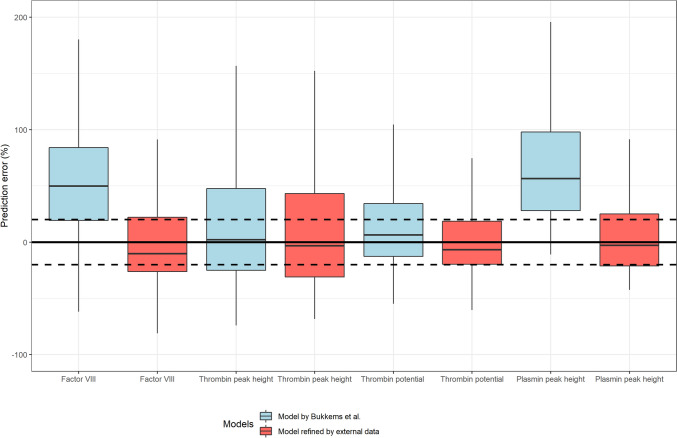
Pharmacokinetic and pharmacodynamic measurements were obtained from 29 severe hemophilia A patients treated with pdVWF/FVIII concentrate (Haemate P). The predictive performance of the previously developed pharmacokinetic-pharmacodynamic model was evaluated using nonlinear mixed-effects modeling (NONMEM). When predictions of FVIII activity or TGA parameters were inadequate [median prediction error (MPE) > 20%], a new model was developed.
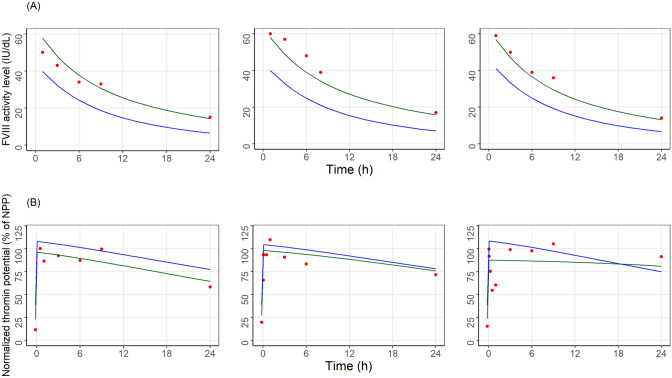
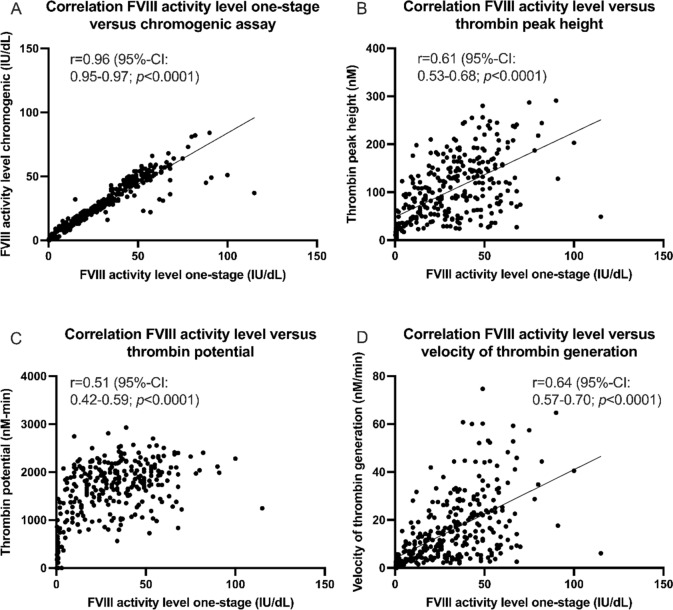
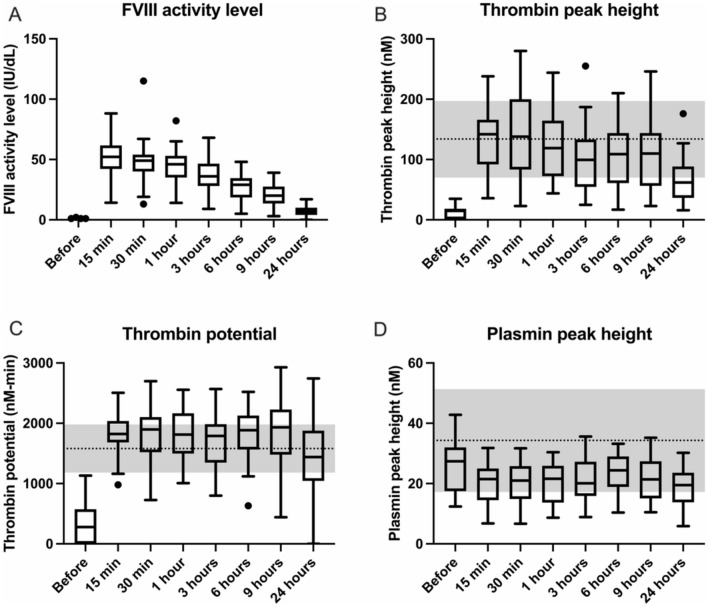
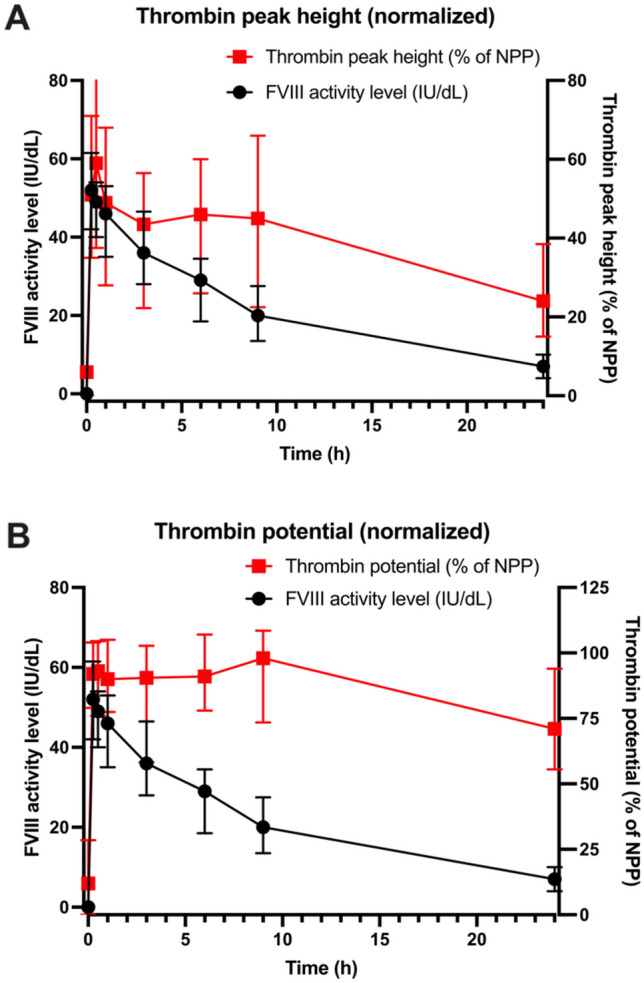
The original pharmacokinetic model underestimated clearance and was refined based on a two-compartment model. The pharmacodynamic model displays no bias in the observed normalized thrombin peak height and normalized thrombin potential (MPE of 6.83% and 7.46%). After re-estimating pharmacodynamic parameters, EC and E values were relatively comparable between the original model and this group. Prediction of normalized plasmin peak height was inaccurate (MPE 58.9%).
Our predictive performance displayed adequate thrombin pharmacodynamic predictions of the original model, but a new pharmacokinetic model was required. The pharmacodynamic model is not factor specific and applicable to multiple factor concentrates. A prospective study is needed to validate the impact of the FVIII dosing pharmacodynamic model on bleeding reduction in patients.
甲型血友病患者预防性使用因子(F)VIII 进行治疗以防止出血。一般来说,剂量和频率基于药代动力学测量。理想情况下,可以根据血栓生成分析(TGA)测量的止血潜力,如尼梅根止血测定法,进行替代剂量调整。
本研究旨在调查先前开发的 FVIII 替代治疗药代动力学-药效学模型的预测性能,该模型将 FVIII 剂量和 FVIII 活性水平与凝血酶和纤溶酶生成参数相关联。
对 29 名接受 pdVWF/FVIII 浓缩物(Haemate P)治疗的重度甲型血友病 A 患者进行了药代动力学和药效学测量。使用非线性混合效应模型(NONMEM)评估先前开发的药代动力学-药效学模型的预测性能。当 FVIII 活性或 TGA 参数的预测结果不充分[中位数预测误差(MPE)>20%]时,开发了一个新模型。
原始药代动力学模型低估了清除率,并根据两室模型进行了修正。药效学模型对观察到的正常化凝血酶峰值高度和正常化凝血酶潜能没有偏差(MPE 分别为 6.83%和 7.46%)。重新估计药效学参数后,原始模型和该组的 EC 和 E 值相对可比。正常化纤溶酶峰值高度的预测不准确(MPE 为 58.9%)。
我们的预测性能显示了原始模型对凝血酶药效学的预测基本准确,但需要一个新的药代动力学模型。药效学模型不是因子特异性的,适用于多种因子浓缩物。需要前瞻性研究来验证 FVIII 给药药效学模型对患者出血减少的影响。