School of Life Course & Population Sciences Faculty of Life Sciences & Medicine, King's College London London United Kingdom.
Health Economics Research Centre, Nuffield Department of Population Health University of Oxford Oxford United Kingdom.
J Am Heart Assoc. 2024 Mar 5;13(5):e030058. doi: 10.1161/JAHA.123.030058. Epub 2024 Feb 23.
Genetic-guided pharmacotherapy (PGx) is not recommended in clinical guidelines for coronary artery disease (CAD). We aimed to examine the extent and quality of evidence from economic evaluations of PGx in CAD and to identify variables influential in changing conclusions on cost-effectiveness.
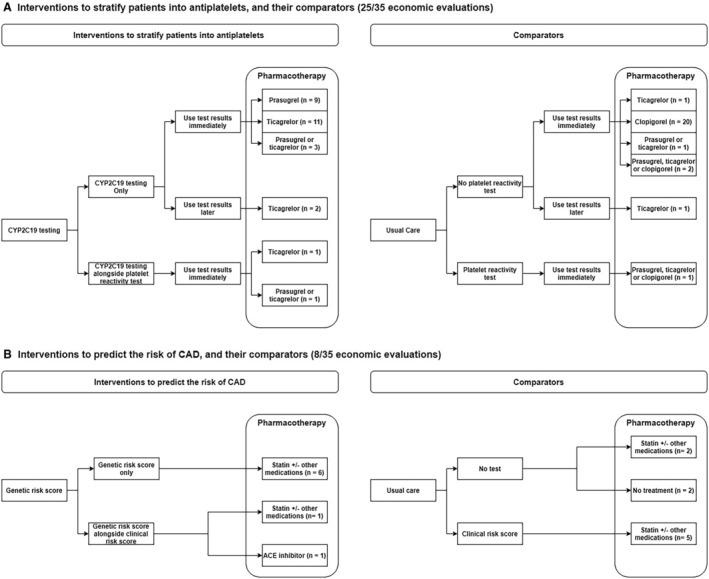
From systematic searches across 6 databases, 2 independent reviewers screened, included, and rated the methodological quality of economic evaluations of PGx testing to guide pharmacotherapy for patients with CAD. Of 35 economic evaluations included, most were model-based cost-utility analyses alone, or alongside cost-effectiveness analyses of PGx testing to stratify patients into antiplatelets (25/35), statins (2/35), pain killers (1/35), or angiotensin-converting enzyme inhibitors (1/35) to predict CAD risk (8/35) or to determine the coumadin doses (1/35). To stratify patients into antiplatelets (96/151 comparisons with complete findings of PGx versus non-PGx), PGx was more effective and more costly than non-PGx clopidogrel (28/43) but less costly than non-PGx prasugrel (10/15) and less costly and less effective than non-PGx ticagrelor (22/25). To predict CAD risk (51/151 comparisons), PGx using genetic risk scores was more effective and less costly than clinical risk score (13/17) but more costly than no risk score (16/19) or no treatment (9/9). The remaining comparisons were too few to observe any trend. Mortality risk was the most common variable (47/294) changing conclusions.
Economic evaluations to date found PGx to stratify patients with CAD into antiplatelets or to predict CAD risk to be cost-effective, but findings varied based on the non-PGx comparators, underscoring the importance of considering local practice in deciding whether to adopt PGx.
基因指导的药物治疗(PGx)在冠心病(CAD)的临床指南中不被推荐。我们旨在研究来自 CAD 中 PGx 的经济评估的证据的范围和质量,并确定影响成本效益变化结论的变量。
从 6 个数据库的系统搜索中,2 名独立审查员筛选、纳入并评估了用于指导 CAD 患者药物治疗的 PGx 检测的经济评估的方法学质量。在纳入的 35 项经济评估中,大多数是基于模型的成本效益分析,或者是与 PGx 检测的成本效益分析一起进行,以将患者分层为抗血小板药物(25/35)、他汀类药物(2/35)、止痛药(1/35)或血管紧张素转换酶抑制剂(1/35),以预测 CAD 风险(8/35)或确定华法林剂量(1/35)。为了将患者分层为抗血小板药物(96/151 项具有完整 PGx 与非 PGx 结果的比较),PGx 比非 PGx 氯吡格雷更有效且更昂贵(28/43),但比非 PGx 普拉格雷更便宜(10/15),比非 PGx 替格瑞洛更便宜且效果更差(22/25)。为了预测 CAD 风险(51/151 项比较),使用遗传风险评分的 PGx 比临床风险评分更有效且成本更低(13/17),但比无风险评分(16/19)或无治疗(9/9)更昂贵。其余的比较数量太少,无法观察到任何趋势。死亡率是最常见的变量(47/294),改变了结论。
迄今为止的经济评估发现,PGx 可以将 CAD 患者分层为抗血小板药物,或者预测 CAD 风险具有成本效益,但结果因非 PGx 对照物而异,这突显了在决定是否采用 PGx 时考虑当地实践的重要性。