Department of Laboratory Medicine, Kumamoto University Hospital, Kumamoto, Japan.
Department of Cardiovascular Medicine, Graduate School of Medical Sciences, Kumamoto University, Kumamoto, Japan.
ESC Heart Fail. 2024 Jun;11(3):1612-1624. doi: 10.1002/ehf2.14710. Epub 2024 Feb 23.
There are minimal data on the prognostic impact of right atrial strain during the reservoir phase (RASr) in patients with immunoglobulin light-chain (AL) cardiac amyloidosis.
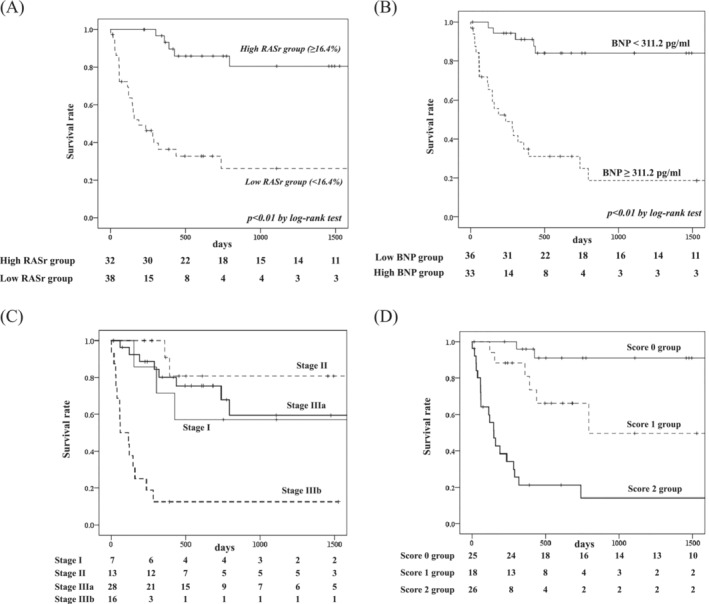
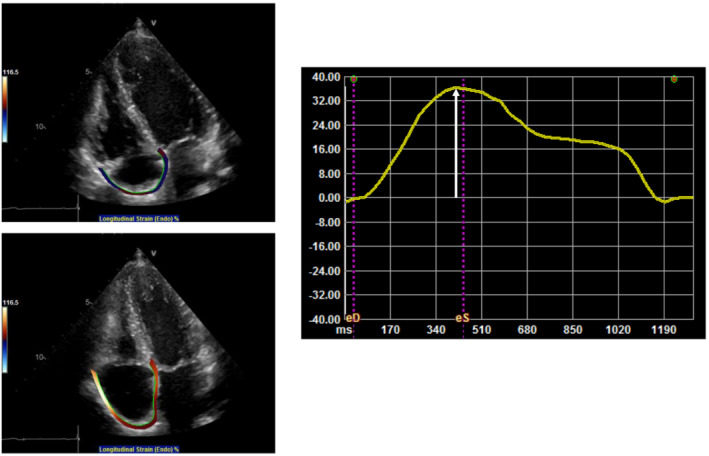
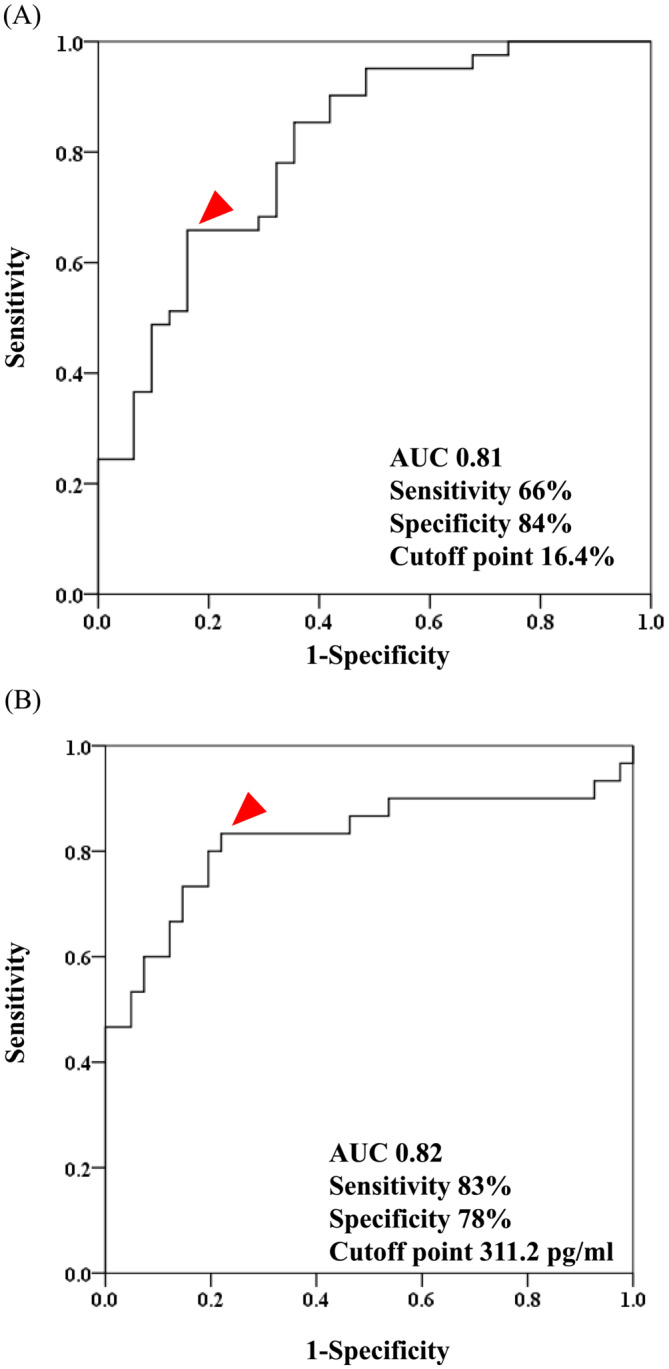
Among 78 patients who were diagnosed with AL cardiac amyloidosis at Kumamoto University Hospital from 2007 to 2022, 72 patients with sufficient two-dimensional speckle tracking imaging data without chemotherapy before the diagnosis were retrospectively analysed. During a median follow-up of 403 days, 31 deaths occurred. Age and the rate of male sex were not significantly different between the all-cause death group and the survival group (age, 70.4 ± 8.8 years vs. 67.0 ± 10.0 years, P = 0.14, male sex, 65% vs. 66%, P = 0.91). The estimated glomerular filtration rate (eGFR) was significantly lower, and B-type natriuretic peptide (BNP) and high sensitivity cardiac troponin T (hs-cTnT) were significantly higher, in the all-cause death group versus the survival group (eGFR, 48.2 ± 21.0 mL/min/1.73 m vs. 59.4 ± 24.4 mL/min/1.73 m, P < 0.05, BNP, 725 [360-1312] pg/mL vs. 123 [81-310] pg/mL, P < 0.01, hs-cTnT, 0.12 [0.07-0.18] ng/mL vs. 0.05 [0.03-0.08] ng/mL, P < 0.01). Left ventricular (LV) global longitudinal strain (GLS) (LV-GLS), left atrial strain during the reservoir phase (LASr), right ventricular GLS (RV-GLS), and RASr were significantly lower in the all-cause death group versus the survival group (LV-GLS, 8.5 ± 4.3% vs. 11.8 ± 3.8%, P < 0.01, LASr, 8.8 ± 7.1% vs. 14.3 ± 8.1%, P < 0.01, RV-GLS, 11.6 ± 5.1% vs. 16.4 ± 3.9%, P < 0.01, RASr, 10.2 ± 7.3% vs. 20.7 ± 9.5%, P < 0.01). RASr was significantly associated with all-cause death after adjusting for RV-GLS, LV-GLS and LASr (hazard ratio [HR]: 0.91, 95% confidence interval [95% CI]: 0.83-0.99, P < 0.05). RASr and log-transformed BNP were significantly associated with all-cause death after adjusting for log-transformed troponin T and eGFR (RASr, HR: 0.93, 95% CI: 0.87-1.00, P < 0.05; log-transformed BNP, HR: 2.10, 95% CI: 1.17-3.79, P < 0.05). The optimal cut-off values were RASr: 16.4% (sensitivity: 66%, specificity: 84%, area under curve [AUC]: 0.81) and BNP: 311.2 pg/mL (sensitivity: 83%, specificity: 78%, AUC: 0.82) to predict all-cause mortality using ROC analysis. Kaplan-Meier analysis revealed that patients with low RASr (<16.4%) or high BNP (>311.2 pg/mL) had a significantly high probability of all-cause death (both, P < 0.01). We devised a new staging score by adding 1 point if RASr decreased or BNP levels increased more than each cut-off value. The HR for all-cause death using score 0 as a reference was 5.95 (95% CI: 1.19-29.79; P < 0.05) for score 1 and 23.29 (95% CI: 5.37-100.98; P < 0.01) for score 2.
The new staging system using RASr and BNP predicted prognosis in patients with AL cardiac amyloidosis.
在免疫球蛋白轻链(AL)心脏淀粉样变性患者中,储存期右房应变(RASr)对预后的影响数据很少。
在 2007 年至 2022 年期间,熊本大学医院诊断出 78 例 AL 心脏淀粉样变性患者,回顾性分析了 72 例具有足够二维斑点追踪成像数据且在诊断前未接受化疗的患者。在中位随访 403 天期间,31 例患者死亡。全因死亡组和存活组的年龄和男性比例无显著差异(年龄,70.4±8.8 岁 vs. 67.0±10.0 岁,P=0.14,男性比例,65% vs. 66%,P=0.91)。全因死亡组的估计肾小球滤过率(eGFR)明显较低,B 型利钠肽(BNP)和高敏心肌肌钙蛋白 T(hs-cTnT)明显较高(eGFR,48.2±21.0 mL/min/1.73 m 比 59.4±24.4 mL/min/1.73 m,P<0.05,BNP,725[360-1312] pg/mL 比 123[81-310] pg/mL,P<0.01,hs-cTnT,0.12[0.07-0.18] ng/mL 比 0.05[0.03-0.08] ng/mL,P<0.01)。左心室(LV)整体纵向应变(GLS)(LV-GLS)、储存期左房应变(LASr)、右心室 GLS(RV-GLS)和 RASr 均明显低于全因死亡组(LV-GLS,8.5±4.3% vs. 11.8±3.8%,P<0.01,LASr,8.8±7.1% vs. 14.3±8.1%,P<0.01,RV-GLS,11.6±5.1% vs. 16.4±3.9%,P<0.01,RASr,10.2±7.3% vs. 20.7±9.5%,P<0.01)。在调整 RV-GLS、LV-GLS 和 LASr 后,RASr 与全因死亡显著相关(风险比[HR]:0.91,95%置信区间[95%CI]:0.83-0.99,P<0.05)。在调整 log 转化后的肌钙蛋白 T 和 eGFR 后,RASr 和 log 转化后的 BNP 与全因死亡显著相关(RASr,HR:0.93,95%CI:0.87-1.00,P<0.05;log 转化后的 BNP,HR:2.10,95%CI:1.17-3.79,P<0.05)。ROC 分析的最佳截断值为 RASr:16.4%(灵敏度:66%,特异性:84%,曲线下面积[AUC]:0.81)和 BNP:311.2 pg/mL(灵敏度:83%,特异性:78%,AUC:0.82),用于预测全因死亡率。Kaplan-Meier 分析显示,RASr 低(<16.4%)或 BNP 高(>311.2 pg/mL)的患者全因死亡的概率显著较高(均,P<0.01)。我们通过增加 RASr 降低或 BNP 水平超过每个截断值加 1 分的方式制定了一个新的分期评分。以评分 0 为参考,评分 1 的全因死亡风险比(HR)为 5.95(95%CI:1.19-29.79;P<0.05),评分 2 的 HR 为 23.29(95%CI:5.37-100.98;P<0.01)。
使用 RASr 和 BNP 的新分期系统预测了 AL 心脏淀粉样变性患者的预后。