Division of Pancreatic Surgery, IRCCS Azienda Ospedaliero-Universitaria Di Bologna, Bologna, Italy.
Department of Internal Medicine and Surgery (DIMEC); Alma Mater Studiorum, University of Bologna, Bologna, Italy.
Ann Surg Oncol. 2024 May;31(5):2943-2950. doi: 10.1245/s10434-024-14959-w. Epub 2024 Feb 24.
The superiority of early drain removal (EDR) versus late (LDR) after pancreaticoduodenectomy (PD) has been demonstrated only in RCTs.
A meta-analysis was conducted using a random-effects model and trial sequential analysis. The critical endpoints were morbidity, redrainage, relaparotomy, and postoperative pancreatic fistula (CR-POPF). Hemorrhage (PPH), delayed gastric emptying (DGE), length of stay (LOS), and readmission rates were also evaluated. Risk ratios (RRs) and mean differences (MDs) with a 95% confidence interval (CI) were calculated. Type I and type II errors were excluded, comparing the accrued sample size (ASS) with the required sample size (RIS). When RIS is superior to ASS, type I or II errors can be hypothesized.
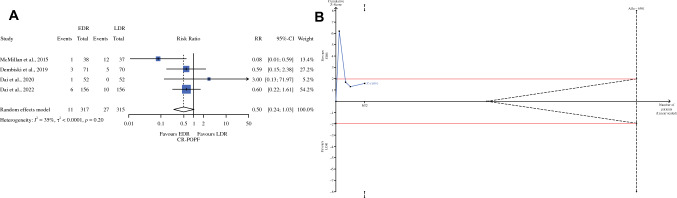
ASS was 632 for all endpoints except DGE and PPH (557 patients). The major morbidity (RR 0.55; 95% CI 0.32-0.97) was lower in the EDR group. The CR-POPF rate was lower in the EDR than in the LDR group (RR 0.50), but this difference is not statistically significant (95% CI 0.24-1.03). The RIS to confirm or exclude these results can be reached by randomizing 5959 patients. The need for percutaneous drainage, relaparotomy, PPH, DGE, and readmission rates was similar. The related RISs were higher than ASS, and type II errors cannot be excluded. LOS was shorter in the EDR than the LDR group (MD - 2.25; 95% CI - 3.23 to - 1.28). The RIS was 567, and type I errors can be excluded.
EDR, compared with LDR, is associated with lower major morbidity and shorter LOS.
只有 RCT 证实了胰十二指肠切除术后(PD)早期引流拔除(EDR)优于晚期引流拔除(LDR)。
使用随机效应模型和试验序贯分析进行荟萃分析。主要终点为发病率、再引流、再次剖腹手术和术后胰腺瘘(CR-POPF)。还评估了出血(PPH)、胃排空延迟(DGE)、住院时间(LOS)和再入院率。计算风险比(RR)和均数差(MD)及 95%置信区间(CI)。排除Ⅰ型和Ⅱ型错误,将累积样本量(ASS)与所需样本量(RIS)进行比较。当 RIS 优于 ASS 时,可以假设存在Ⅰ型或Ⅱ型错误。
除 DGE 和 PPH 外(557 例患者),所有终点的 ASS 均为 632 例。EDR 组的主要发病率(RR 0.55;95%CI 0.32-0.97)较低。EDR 组的 CR-POPF 发生率低于 LDR 组(RR 0.50),但无统计学意义(95%CI 0.24-1.03)。通过随机分配 5959 例患者可以达到确认或排除这些结果的 RIS。需要经皮引流、再次剖腹手术、PPH、DGE 和再入院率相似。相关 RIS 高于 ASS,不能排除Ⅱ型错误。EDR 组的 LOS 短于 LDR 组(MD -2.25;95%CI -3.23 至 -1.28)。RIS 为 567,可以排除Ⅰ型错误。
与 LDR 相比,EDR 与较低的主要发病率和较短的 LOS 相关。