Gong Yusi, Song Yang, Xu Jiaman, Dong Huaying, Orkaby Ariela R, Kramer Daniel B, Dodson John A, Strom Jordan B
Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology, Beth Israel Deaconess Medical Center, Boston, MA, USA.
Brigham and Women's Hospital, Division on Aging, Boston, MA, USA.
medRxiv. 2024 Feb 13:2024.02.09.24302612. doi: 10.1101/2024.02.09.24302612.
Frailty is associated with adverse cardiovascular outcomes independent of age and comorbidities, yet the independent influence of frailty progression remains uncertain.
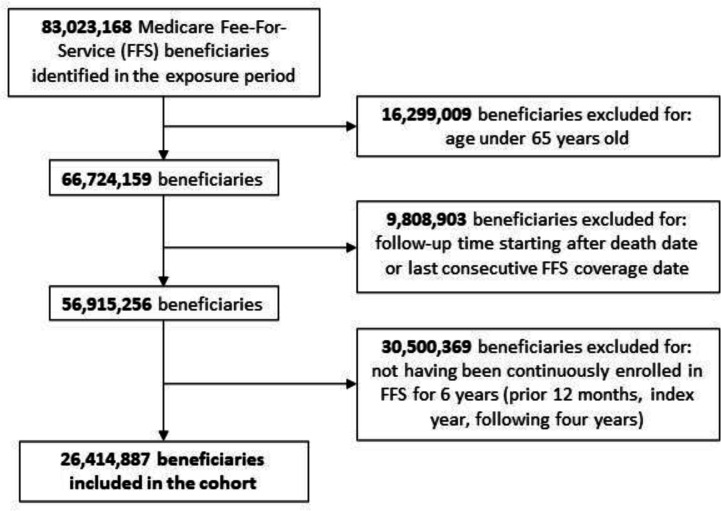
Medicare Fee-for-service beneficiaries ≥ 65 years at cohort inception with continuous enrollment from 2003-2015 were included. Frailty trajectory was measured by annualized change in a validated claims-based frailty index (CFI) over a 5-year period. Linear mixed effects models, adjusting for baseline frailty, were used to estimate CFI change over a 5-year period. Survival analysis was used to evaluate associations of frailty progression and future health outcomes (major adverse cardiovascular and cerebrovascular events [MACCE], all-cause death, heart failure, myocardial infarction, ischemic stroke, and days alive at home [DAH] within the following calendar year).
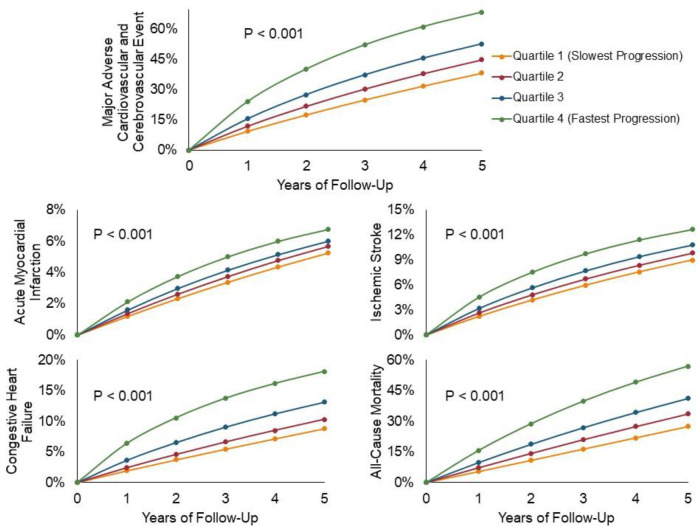
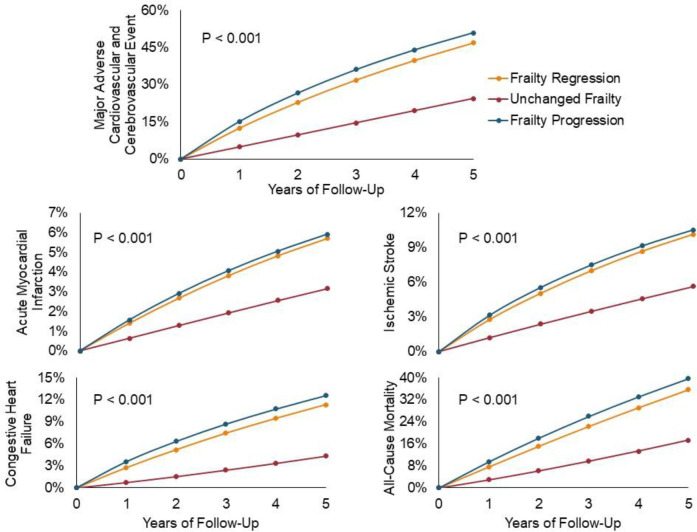
26.4 million unique beneficiaries were included (mean age 75.4 ± 7.0 years, 57% female, 13% non-White). In total, 20% had frailty progression, 66% had no change in frailty, and 14% frailty regression over median follow-up of 2.4 years. Compared to those without a change in CFI, when adjusting for baseline frailty, those with frailty progression had significantly greater risk of incident MACCE (hazard ratio [HR] 2.30, 95% confidence interval [CI] 2.30-2.31), all-cause mortality (HR 1.59, 95% CI 1.58-1.59), acute myocardial infarction (HR 1.78, 95% CI 1.77-1.79), heart failure (HR 2.78, 95% CI 2.77-2.79), and stroke (HR 1.78, 95% CI 1.77-1.79). There was also a graded increase in risk of each outcome with more rapid progression and significantly fewer DAH with the most rapid vs. the slowest progression group (270.4 ± 112.3 vs. 308.6 ± 93.0 days, rate ratio 0.88, 95% CI 0.87-0.88, p < 0.001).
In this large, nationwide sample of Medicare beneficiaries, frailty progression, independent of baseline frailty, was associated with fewer DAH and a graded risk of MACCE, all-cause mortality, myocardial infarction, heart failure, and stroke compared to those without progression.
虚弱与不良心血管结局相关,独立于年龄和合并症之外,然而虚弱进展的独立影响仍不确定。
纳入队列起始时年龄≥65岁且在2003年至2015年连续参保的医疗保险按服务付费受益人。虚弱轨迹通过在5年期间基于验证后的索赔虚弱指数(CFI)的年化变化来衡量。使用线性混合效应模型,并对基线虚弱进行调整,以估计5年期间CFI的变化。生存分析用于评估虚弱进展与未来健康结局(主要不良心血管和脑血管事件[MACCE]、全因死亡、心力衰竭、心肌梗死、缺血性中风以及下一年度在家存活天数[DAH])之间的关联。
纳入2640万独特受益人(平均年龄75.4±7.0岁,57%为女性,13%为非白人)。在中位随访2.4年期间,总计20%有虚弱进展,66%虚弱无变化,14%虚弱逆转。与CFI无变化者相比,在调整基线虚弱后,虚弱进展者发生MACCE(风险比[HR]2.30,95%置信区间[CI]2.30 - 2.31)、全因死亡率(HR 1.59,95% CI 1.58 - 1.59)、急性心肌梗死(HR 1.78,95% CI 1.77 - 1.79)、心力衰竭(HR 2.78,95% CI 2.77 - 2.79)和中风(HR 1.78,95% CI 1.77 - 1.79)的风险显著更高。随着进展速度加快,各结局风险呈分级增加,进展最快组与最慢组相比,在家存活天数显著减少(270.4±112.3天对308.6±93.0天,率比0.88,95% CI 0.87 - 0.88,p < 0.001)。
在这个大型全国性医疗保险受益人群样本中,与无进展者相比,独立于基线虚弱的虚弱进展与在家存活天数减少以及MACCE、全因死亡率、心肌梗死、心力衰竭和中风的分级风险相关。