British Columbia Centre for Disease Control, V5Z 4R4, Vancouver, BC, Canada.
School of Population and Public Health, University of British Columbia, V6T 1Z4, Vancouver, BC, Canada.
BMC Infect Dis. 2024 Feb 26;24(1):262. doi: 10.1186/s12879-024-09067-9.
Widespread human-to-human transmission of the severe acute respiratory syndrome coronavirus two (SARS-CoV-2) stems from a strong affinity for the cellular receptor angiotensin converting enzyme two (ACE2). We investigate the relationship between a patient's nasopharyngeal ACE2 transcription and secondary transmission within a series of concurrent hospital associated SARS-CoV-2 outbreaks in British Columbia, Canada.
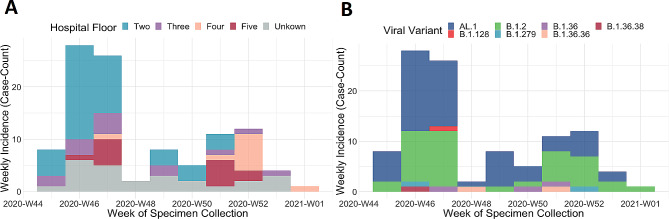
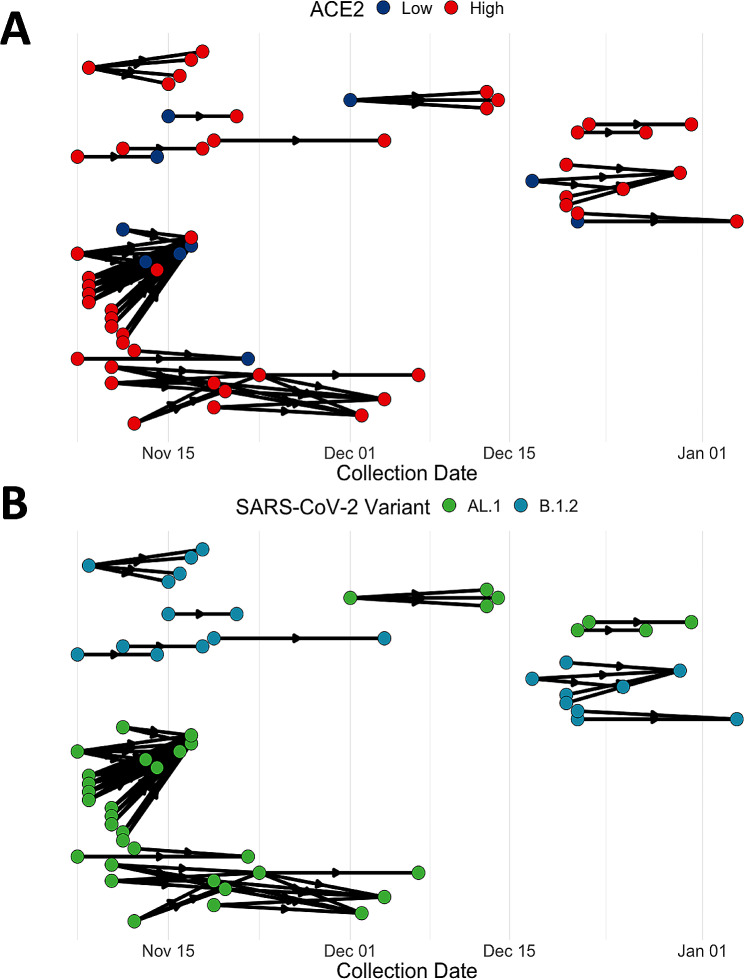
Epidemiological case data from the outbreak investigations was merged with public health laboratory records and viral lineage calls, from whole genome sequencing, to reconstruct the concurrent outbreaks using infection tracing transmission network analysis. ACE2 transcription and RNA viral load were measured by quantitative real-time polymerase chain reaction. The transmission network was resolved to calculate the number of potential secondary cases. Bivariate and multivariable analyses using Poisson and Negative Binomial regression models was performed to estimate the association between ACE2 transcription the number of SARS-CoV-2 secondary cases.
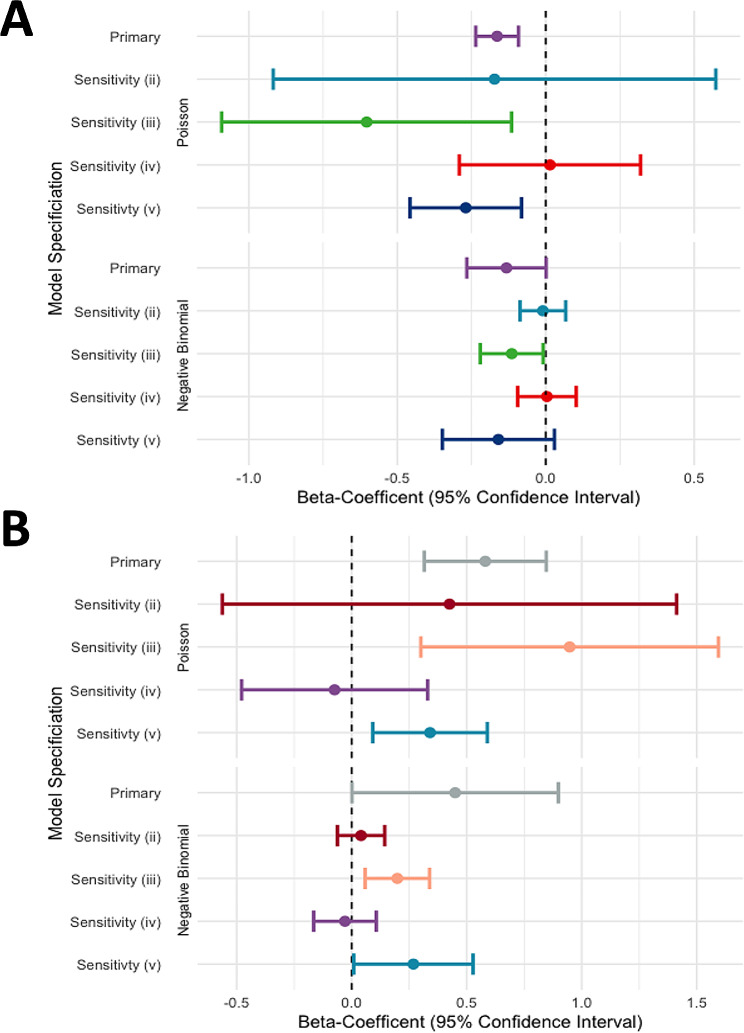
The infection tracing transmission network provided n = 76 potential transmission events across n = 103 cases. Bivariate comparisons found that on average ACE2 transcription did not differ between patients and healthcare workers (P = 0.86). High ACE2 transcription was observed in 98.6% of transmission events, either the primary or secondary case had above average ACE2. Multivariable analysis found that the association between ACE2 transcription (log fold-change) and the number of secondary transmission events differs between patients and healthcare workers. In health care workers Negative Binomial regression estimated that a one-unit change in ACE2 transcription decreases the number of secondary cases (β = -0.132 (95%CI: -0.255 to -0.0181) adjusting for RNA viral load. Conversely, in patients a one-unit change in ACE2 transcription increases the number of secondary cases (β = 0.187 (95% CI: 0.0101 to 0.370) adjusting for RNA viral load. Sensitivity analysis found no significant relationship between ACE2 and secondary transmission in health care workers and confirmed the positive association among patients.
Our study suggests that ACE2 transcription has a positive association with SARS-CoV-2 secondary transmission in admitted inpatients, but not health care workers in concurrent hospital associated outbreaks, and it should be further investigated as a risk-factor for viral transmission.
严重急性呼吸综合征冠状病毒 2 型(SARS-CoV-2)在人与人之间广泛传播,源于其对细胞受体血管紧张素转换酶 2(ACE2)的强烈亲和力。我们调查了一系列同时发生的不列颠哥伦比亚省加拿大医院相关 SARS-CoV-2 暴发中,患者鼻咽 ACE2 转录与二次传播之间的关系。
从暴发调查的流行病学病例数据中,与公共卫生实验室记录和全基因组测序的病毒谱系调用合并,使用感染追踪传播网络分析来重建同时发生的暴发。通过定量实时聚合酶链反应测量 ACE2 转录和 RNA 病毒载量。解析传播网络以计算潜在的二次病例数。使用泊松和负二项式回归模型进行双变量和多变量分析,以估计 ACE2 转录与 SARS-CoV-2 二次病例数之间的关联。
感染追踪传播网络提供了 n = 103 例患者中的 n = 76 个潜在传播事件。双变量比较发现,患者和医护人员之间的 ACE2 转录平均值没有差异(P = 0.86)。高 ACE2 转录在 98.6%的传播事件中观察到,无论是原发性还是继发性病例,ACE2 均高于平均水平。多变量分析发现,ACE2 转录(对数倍变化)与二次传播事件数量之间的关联在患者和医护人员之间有所不同。在医护人员中,负二项式回归估计 ACE2 转录的一个单位变化会减少二次病例数(β = -0.132(95%CI:-0.255 至 -0.0181),调整 RNA 病毒载量。相反,在患者中,ACE2 转录的一个单位变化会增加二次病例数(β = 0.187(95%CI:0.0101 至 0.370),调整 RNA 病毒载量。敏感性分析未发现 ACE2 与医护人员二次传播之间存在显著关系,并证实了患者之间的正相关关系。
我们的研究表明,ACE2 转录与住院患者同时发生的医院相关 SARS-CoV-2 二次传播呈正相关,但与医护人员无关,应进一步作为病毒传播的危险因素进行研究。