Lu Yuan, Keeley Ellen C, Barrette Eric, Cooper-DeHoff Rhonda M, Dhruva Sanket S, Gaffney Jenny, Gamble Ginger, Handke Bonnie, Huang Chenxi, Krumholz Harlan, Rowe Caitrin, Schulz Wade, Shaw Kathryn, Smith Myra, Woodard Jennifer, Young Patrick, Ervin Keondae, Ross Joseph
Yale School of Medicine.
University of Florida.
Res Sq. 2024 Feb 15:rs.3.rs-3943912. doi: 10.21203/rs.3.rs-3943912/v1.
Improving hypertension control is a public health priority. However, consistent identification of uncontrolled hypertension using computable definitions in electronic health records (EHR) across health systems remains uncertain.
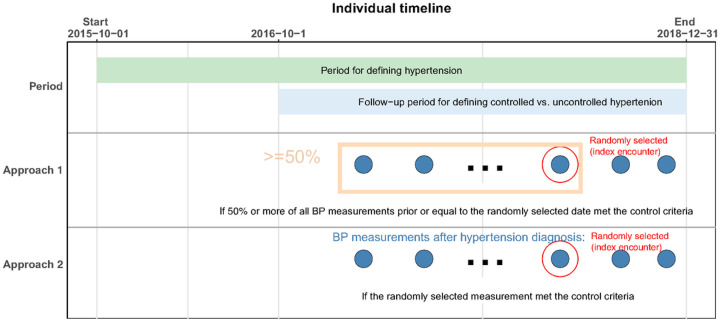
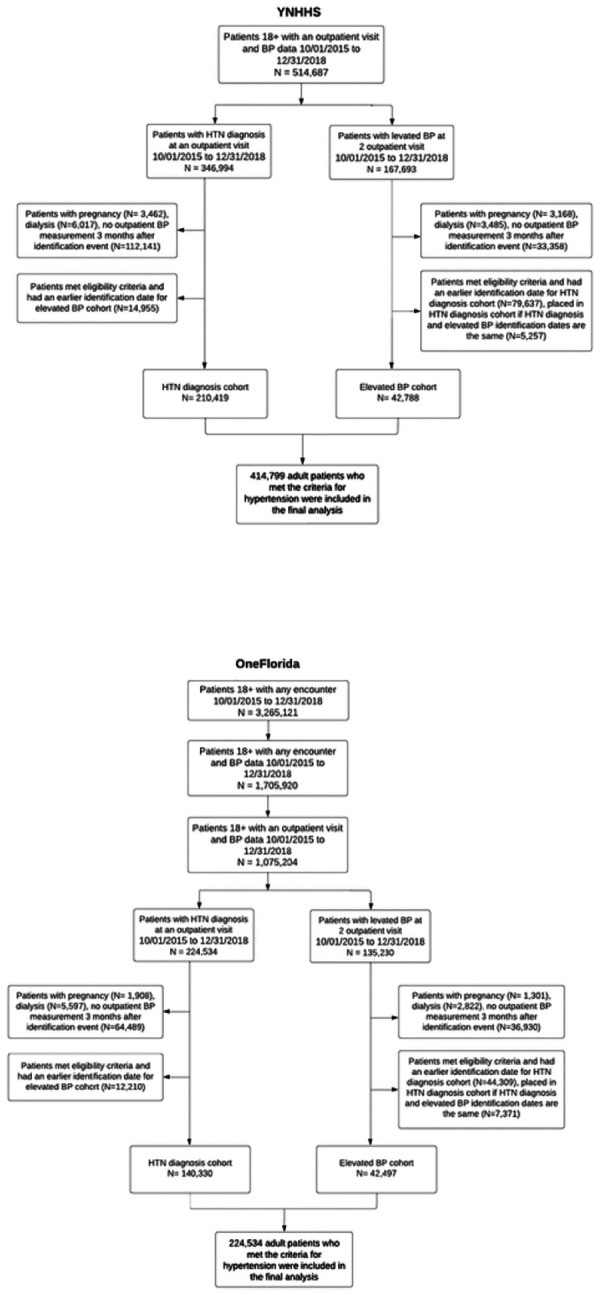
In this retrospective cohort study, we applied two computable definitions to the EHR data to identify patients with controlled and uncontrolled hypertension and to evaluate differences in characteristics, treatment, and clinical outcomes between these patient populations. We included adult patients (≥ 18 years) with hypertension receiving ambulatory care within Yale-New Haven Health System (YNHHS; a large US health system) and OneFlorida Clinical Research Consortium (OneFlorida; a Clinical Research Network comprised of 16 health systems) between October 2015 and December 2018. We identified patients with controlled and uncontrolled hypertension based on either a single blood pressure (BP) measurement from a randomly selected visit or all BP measurements recorded between hypertension identification and the randomly selected visit).
Overall, 253,207 and 182,827 adults at YNHHS and OneFlorida were identified as having hypertension. Of these patients, 83.1% at YNHHS and 76.8% at OneFlorida were identified using ICD-10-CM codes, whereas 16.9% and 23.2%, respectively, were identified using elevated BP measurements (≥ 140/90 mmHg). Uncontrolled hypertension was observed among 32.5% and 43.7% of patients at YNHHS and OneFlorida, respectively. Uncontrolled hypertension was disproportionately higher among Black patients when compared with White patients (38.9% versus 31.5% in YNHHS; p < 0.001; 49.7% versus 41.2% in OneFlorida; p < 0.001). Medication prescription for hypertension management was more common in patients with uncontrolled hypertension when compared with those with controlled hypertension (overall treatment rate: 39.3% versus 37.3% in YNHHS; p = 0.04; 42.2% versus 34.8% in OneFlorida; p < 0.001). Patients with controlled and uncontrolled hypertension had similar rates of short-term (at 3 and 6 months) and long-term (at 12 and 24 months) clinical outcomes. The two computable definitions generated consistent results.
Our findings illustrate the potential of leveraging EHR data, employing computable definitions, to conduct effective digital population surveillance in the realm of hypertension management.
改善高血压控制是一项公共卫生重点工作。然而,在各卫生系统的电子健康记录(EHR)中,使用可计算定义持续识别未得到控制的高血压情况仍不明确。
在这项回顾性队列研究中,我们将两种可计算定义应用于EHR数据,以识别高血压得到控制和未得到控制的患者,并评估这些患者群体在特征、治疗及临床结局方面的差异。我们纳入了2015年10月至2018年12月期间在耶鲁 - 纽黑文医疗系统(YNHHS;美国一个大型医疗系统)和OneFlorida临床研究联盟(OneFlorida;一个由16个卫生系统组成的临床研究网络)接受门诊护理的成年高血压患者(≥18岁)。我们根据从随机选择的就诊中获取的单次血压(BP)测量值,或高血压确诊至随机选择的就诊期间记录的所有BP测量值,来识别高血压得到控制和未得到控制的患者。
总体而言,YNHHS和OneFlorida分别有253,207名和182,827名成年人被确定患有高血压。在这些患者中,YNHHS有83.1%、OneFlorida有76.8%是通过ICD - 10 - CM编码识别出来的,而分别有16.9%和23.2%是通过血压升高测量值(≥140/90 mmHg)识别出来的。YNHHS和OneFlorida分别有32.5%和43.7%的患者存在未得到控制的高血压。与白人患者相比,黑人患者中未得到控制的高血压比例过高(YNHHS中为38.9%对31.5%;p < 0.001;OneFlorida中为49.7%对41.2%;p < 0.001)。与高血压得到控制的患者相比,高血压管理的药物处方在未得到控制的高血压患者中更为常见(总体治疗率:YNHHS中为39.3%对37.3%;p = 0.04;OneFlorida中为42.2%对34.8%;p < 0.001)。高血压得到控制和未得到控制的患者在短期(3个月和6个月)和长期(12个月和24个月)临床结局方面的发生率相似。这两种可计算定义产生了一致的结果。
我们的研究结果表明,利用EHR数据并采用可计算定义在高血压管理领域进行有效的数字人群监测具有潜力。