Liu Kun, Wu Kaisheng, Shen Jinglun, Meng Fei, Nappi Francesco, Alfonso Fernando, Wang Shengxun, Zheng Shuai, Zhang Haibo
Department of Cardiac Surgery, Cardiovascular Medical Center, the University of Hong Kong-Shenzhen Hospital, Shenzhen, China.
Department of Cardiac Surgery, Beijing Anzhen Hospital, Capital Medical University, Beijing, China.
J Thorac Dis. 2024 Jan 30;16(1):593-603. doi: 10.21037/jtd-23-1885. Epub 2024 Jan 22.
Due to the influence of anatomical structure, replacing the bicuspid valve using transcatheter aortic valve replacement (TAVR) would increase the risk of perivalvular leakage and conduction block, affecting the hemodynamic effect of the interventional valve. In this study, for bicuspid and tricuspid valves, we implemented different valve selection strategies to explore the safety and effectiveness of TAVR in the treatment of bicuspid aortic stenosis with "down-size" interventional valves using the VenusA-valve system.
The operation was performed with the VenusA-valve via transfemoral approach. The selected valves were appropriately sized based on the results of transthoracic echocardiography (TTE), contrast-enhanced computed tomography (CT), and the morphology of intraoperative pre-dilation balloons. For tricuspid valve cases, the VenusA valve is usually larger than the annulus diameter, whereas the "down-size" approach was adopted for bicuspid aortic valve (BAV) cases. The shape of the pre-dilation balloon allowed further sizing of the annulus diameter by the degree of lumbar constriction of the balloon, aiding in intervention valve size selection, particularly in cases of BAVs.
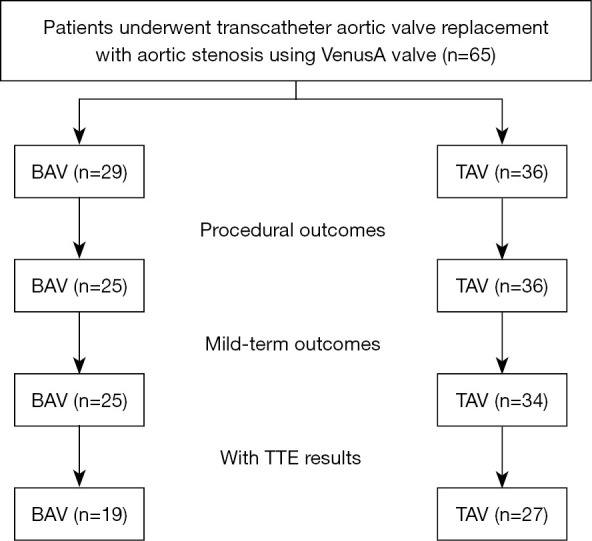
A total of 65 patients underwent TAVR for aortic stenosis with VenusA-valve systems. Of these, 29 cases had a BAV and 36 cases had a tricuspid aortic valve (TAV). The distribution of VenusA-valve sizes differed between TAV and BAV cases (P=0.007). Furthermore, there was a significant decrease in the average mean gradient in TAV patients from 54.7 to 12.2 mmHg (P<0.001), and in BAV patients from 61.6 to 14.3 mmHg (P<0.001). The percentage of paravalvular leakage greater than mild was 6.90% in the BAVs and 5.56% in the TAVs at procedural outcomes (P=0.955). The mean follow-up period was 22.23 months (range, 12 to 39 months). The proportion of New York Heart Association (NYHA) class III/IV decreased from 78.5% preoperatively to 11.3% at the last follow-up (P<0.001). A total of 27 patients with TAV and 19 patients with BAV underwent TTE at 1-year follow-up after operation. There was no significant contrast in the average pressure difference between TAVs and BAVs at 1-year follow-up (11.9 14.3 mmHg, P=0.18).
The VenusA-valve for TAVR produced positive clinical outcomes and valve functionality in both BAVs and TAVs. In the case of BAVs, selecting a smaller interventional valve size was deemed viable.
由于解剖结构的影响,经导管主动脉瓣置换术(TAVR)用于置换二尖瓣会增加瓣周漏和传导阻滞的风险,影响介入瓣膜的血流动力学效果。在本研究中,对于二尖瓣和三尖瓣,我们实施了不同的瓣膜选择策略,以探讨使用VenusA瓣膜系统采用“减径”介入瓣膜治疗二尖瓣主动脉狭窄的TAVR的安全性和有效性。
通过经股动脉途径使用VenusA瓣膜进行手术。根据经胸超声心动图(TTE)、对比增强计算机断层扫描(CT)的结果以及术中预扩张球囊的形态,选择尺寸合适的瓣膜。对于三尖瓣病例,VenusA瓣膜通常大于瓣环直径,而对于二尖瓣主动脉瓣(BAV)病例则采用“减径”方法。预扩张球囊的形状可通过球囊腰部收缩程度进一步确定瓣环直径大小,有助于介入瓣膜尺寸的选择,尤其是在BAV病例中。
共有65例患者使用VenusA瓣膜系统进行了主动脉狭窄的TAVR。其中,29例为BAV,36例为三尖瓣主动脉瓣(TAV)。TAV和BAV病例中VenusA瓣膜尺寸的分布有所不同(P = 0.007)。此外,TAV患者的平均平均梯度从54.7 mmHg显著降至12.2 mmHg(P < 0.001),BAV患者从61.6 mmHg降至14.3 mmHg(P < 0.001)。在手术结果中,BAV中大于轻度的瓣周漏百分比为6.90%,TAV中为5.56%(P = 0.955)。平均随访期为22.23个月(范围12至39个月)。纽约心脏协会(NYHA)III/IV级的比例从术前的78.5%降至最后随访时的11.3%(P < 0.001)。共有27例TAV患者和19例BAV患者在术后1年随访时进行了TTE。在1年随访时,TAV和BAV之间的平均压差无显著差异(11.9±14.3 mmHg,P = 0.18)。
用于TAVR的VenusA瓣膜在BAV和TAV中均产生了积极的临床结果和瓣膜功能。对于BAV病例,选择较小尺寸的介入瓣膜被认为是可行的。