From the Anaesthesia and Intensive Care Department, Raymond Poincaré Hospital, APHP, Garches, France; Université Paris-Saclay, UVSQ, Inserm, LPPD, Boulogne, France (VM), the Center for Clinical Studies, University Hospital, Jena, Germany (TL), the Department of Anesthesiology and Acute Postoperative & Transitional Pain Service, Cliniques Universitaires St Luc - University Catholic of Louvain, Brussels, Belgium (PL), Anaesthesia and Intensive Care Department, Ambroise Paré Hospital, APHP, Boulogne Billancourt, France; Université Paris-Saclay, UVSQ, Inserm, LPPD, Boulogne, France (HK, DF), the Department of Anaesthesiology, Intensive Care and Pain Medicine, Helsinki University Hospital and SleepWell Research Programme, University of Helsinki (EK), the Department of Anaesthesiology, Intensive Care and Pain Medicine, University Hospital Münster UKM, Munster, Germany (EMPZ), the Department of Anaesthesiology and Intensive Care, Jena University Hospital Friedrich Schiller University, Jena, Germany (MK, WM, CW).
Eur J Anaesthesiol. 2024 May 1;41(5):351-362. doi: 10.1097/EJA.0000000000001974. Epub 2024 Feb 27.
Chronic postsurgical pain (CPSP) is a clinical problem, and large prospective studies are needed to determine its incidence, characteristics, and risk factors.
To find predictive factors for CPSP in an international survey.
Observational study.
Multicentre European prospective observational trial.
Patients undergoing breast cancer surgery, sternotomy, endometriosis surgery, or total knee arthroplasty (TKA).
Standardised questionnaires were completed by the patients at 1, 3, and 7 days, and at 1, 3, and 6 months after surgery, with follow-up via E-mail, telephone, or interview.
The primary goal of NIT-1 was to propose a scoring system to predict those patient likely to have CPSP at 6 months after surgery.
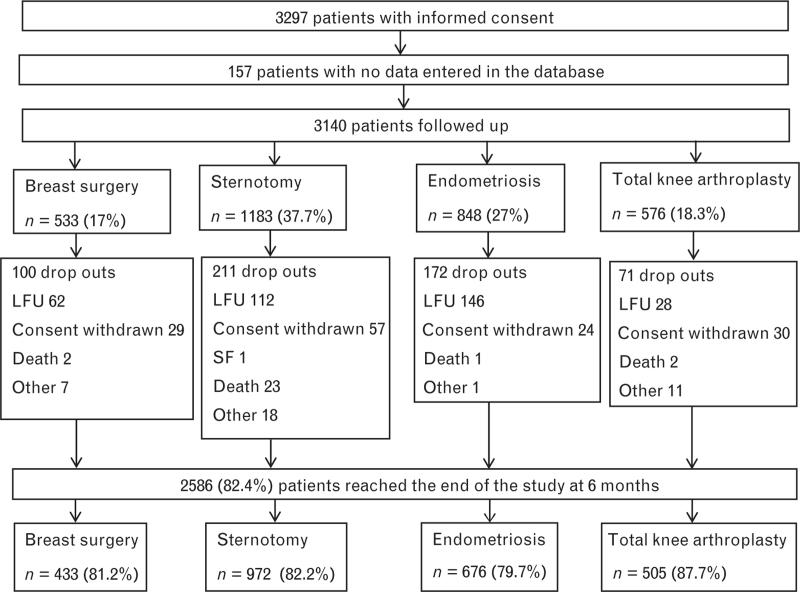
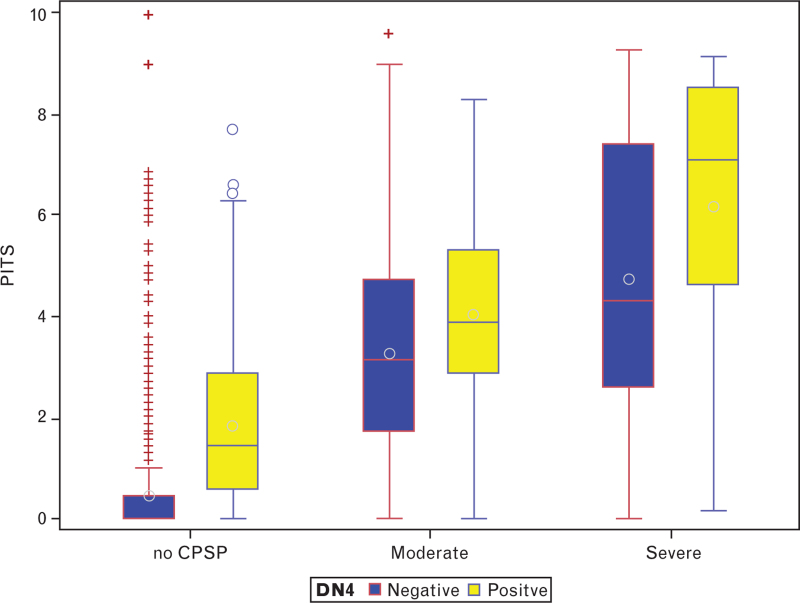
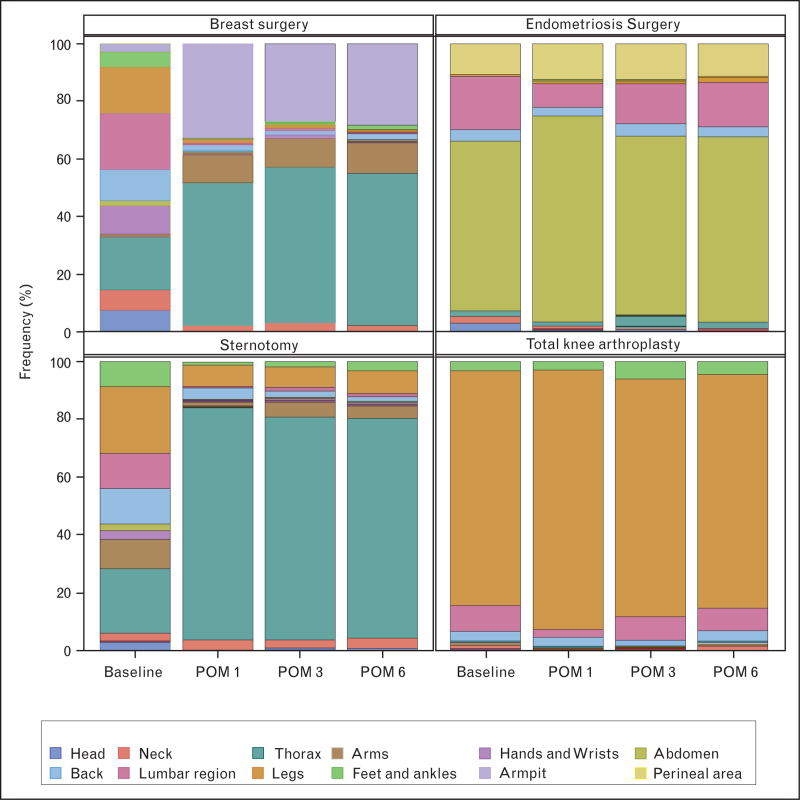
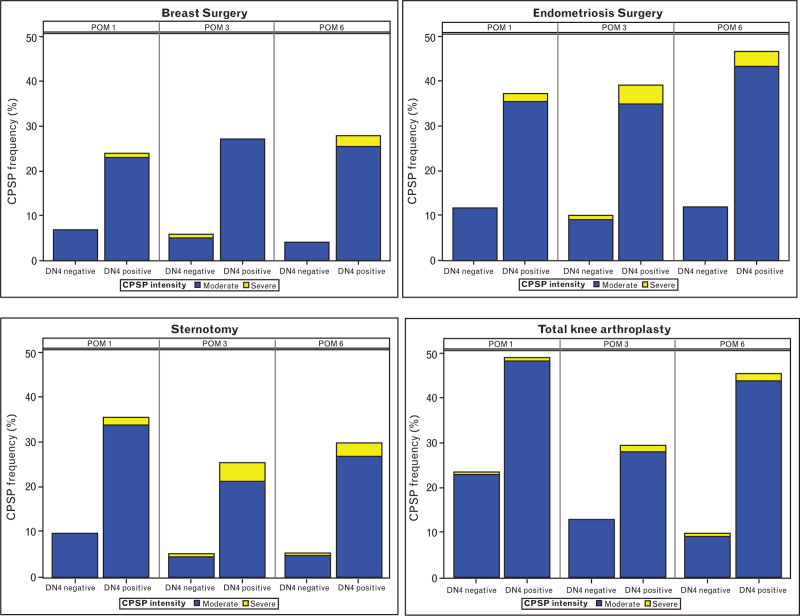
A total of 3297 patients were included from 18 hospitals across Europe and 2494 patients were followed-up for 6 months. The mean incidence of CPSP at 6 months was 10.5%, with variations depending on the type of surgery: sternotomy 6.9%, breast surgery 7.4%, TKA 12.9%, endometriosis 16.2%. At 6 months, neuropathic characteristics were frequent for all types of surgery: sternotomy 33.3%, breast surgery 67.6%, TKA 42.4%, endometriosis 41.4%. One-third of patients experienced CPSP at both 3 and 6 months. Pre-operative pain was frequent for TKA (leg pain) and endometriosis (abdomen) and its frequency and intensity were reduced after surgery. Severe CPSP and a neuropathic pain component decreased psychological and functional wellbeing as well as quality of life. No overarching CPSP risk factors were identified.
Unfortunately, our findings do not offer a new CPSP predictive score. However, we present reliable new data on the incidence, characteristics, and consequences of CPSP from a large European survey. Interesting new data on the time course of CPSP, its neuropathic pain component, and CPSP after endometriosis surgery generate new hypotheses but need to be confirmed by further research.
clinicaltrials.gov ID: NCT03834922.
慢性术后疼痛(CPSP)是一种临床问题,需要进行大型前瞻性研究来确定其发生率、特征和危险因素。
在国际调查中寻找 CPSP 的预测因素。
观察性研究。
多中心欧洲前瞻性观察性试验。
接受乳腺癌手术、胸骨切开术、子宫内膜异位症手术或全膝关节置换术(TKA)的患者。
患者在手术后第 1、3 和 7 天以及第 1、3 和 6 个月时完成标准化问卷,并通过电子邮件、电话或访谈进行随访。
NIT-1 的主要目标是提出一种评分系统,以预测那些在手术后 6 个月时可能患有 CPSP 的患者。
来自欧洲 18 家医院的共 3297 名患者入组,2494 名患者随访 6 个月。6 个月时 CPSP 的平均发生率为 10.5%,手术类型不同发生率有所不同:胸骨切开术 6.9%,乳房手术 7.4%,TKA 12.9%,子宫内膜异位症 16.2%。6 个月时,所有手术类型均有频繁的神经病理性特征:胸骨切开术 33.3%,乳房手术 67.6%,TKA 42.4%,子宫内膜异位症 41.4%。三分之一的患者在 3 个月和 6 个月时均出现 CPSP。TKA(腿部疼痛)和子宫内膜异位症(腹部疼痛)术前疼痛较为常见,术后疼痛减轻。严重的 CPSP 和神经病理性疼痛成分降低了心理和功能健康状况以及生活质量。未确定总体 CPSP 危险因素。
不幸的是,我们的研究结果并未提供新的 CPSP 预测评分。然而,我们从一项大型欧洲调查中提供了关于 CPSP 的发生率、特征和后果的可靠新数据。关于 CPSP 的时间进程、神经病理性疼痛成分以及子宫内膜异位症手术后 CPSP 的有趣新数据提出了新的假说,但需要进一步研究来证实。
clinicaltrials.gov ID:NCT03834922。