Scibilia Antonino, Rustici Arianna, Linari Marta, Zenesini Corrado, Belotti Laura Maria Beatrice, Dall'Olio Massimo, Princiotta Ciro, Cuoci Andrea, Aspide Raffaele, Migliorino Ernesto, Moneti Manuel, Sturiale Carmelo, Castioni Carlo Alberto, Conti Alfredo, Bortolotti Carlo, Cirillo Luigi
IRCCS Istituto delle Scienze Neurologiche di Bologna, UOC Neurochirurgia, Bologna, Italy.
IRCCS Istituto delle Scienze Neurologiche di Bologna, UOSI di Neuroradiologia Ospedale Maggiore, Bologna, Italy.
Front Neurol. 2024 Feb 15;15:1286862. doi: 10.3389/fneur.2024.1286862. eCollection 2024.
The management of patients with poor-grade aneurysmal subarachnoid hemorrhage (aSAH) is burdened by an unfavorable prognosis even with aggressive treatment. The aim of the present study is to investigate the risk factors affecting 30-day mortality in poor-grade aSAH patients.
We performed a retrospective analysis of a prospectively collected database of poor-grade aSAH patients (World Federation of Neurosurgical Societies, WFNS, grades IV and V) treated at our institution from December 2010 to December 2020. For all variables, percentages of frequency distributions were analyzed. Contingency tables (Chi-squared test) were used to assess the association between categorical variables and outcomes in the univariable analysis. Multivariable analysis was performed by using the multiple logistic regression method to estimate the odds ratio (OR) for 30-day mortality.
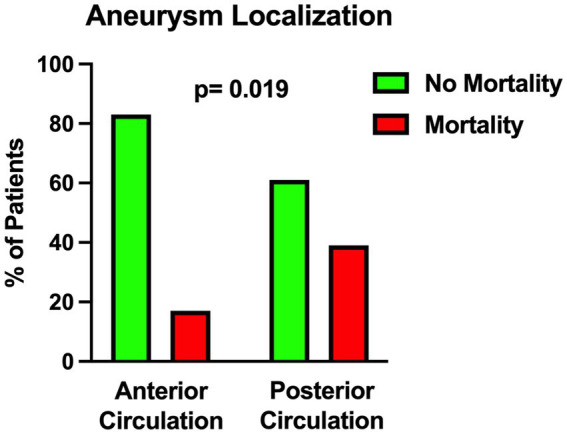
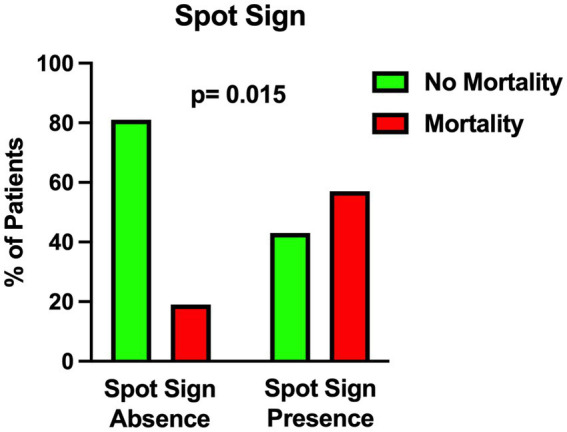
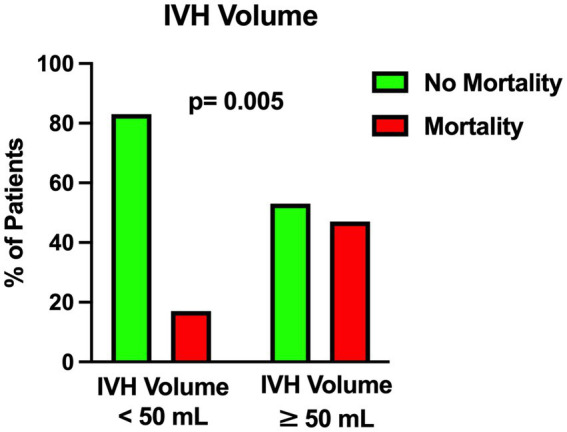
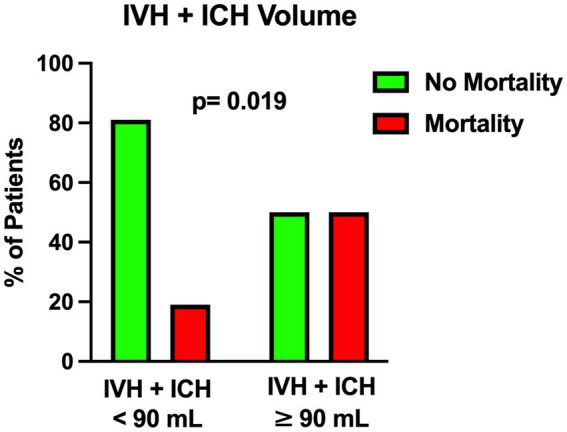
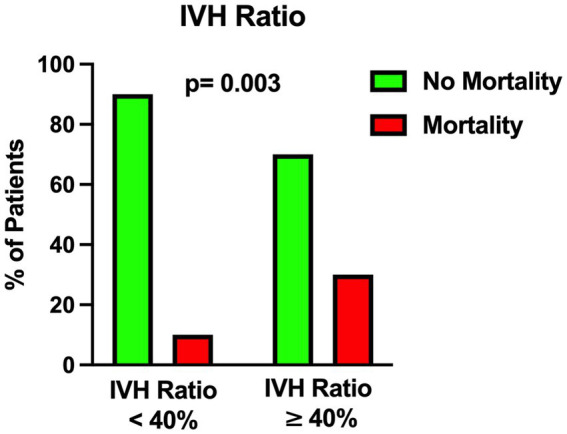
A total of 149 patients were included of which 32% had WFNS grade 4 and 68% had WFNS grade 5. The overall 1-month mortality rate was 21%. On univariable analysis, five variables were found to be associated with the likelihood of death, including intraventricular hemorrhage (IVH ≥ 50 mL, = 0.005), the total amount of intraventricular and intraparenchymal hemorrhage (IVH + ICH ≥ 90 mL, = 0.019), the IVH Ratio (IVH Ratio ≥ 40%, = 0.003), posterior circulation aneurysms ( = 0.019), presence of spot sign on initial CT scan angiography ( = 0.015).Nonetheless, when the multivariable analysis was performed, only IVH Ratio ( = 0.005; OR 3.97), posterior circulation aneurysms ( = 0.008; OR 4.05) and spot sign ( = 0.022; OR 6.87) turned out to be independent predictors of 30-day mortality.
The risk of mortality in poor-grade aSAH remains considerable despite maximal treatment. Notwithstanding the limitations of a retrospective study, our report highlights some neuroradiological features that in the emergency setting, combined with leading clinical and anamnestic parameters, may support the multidisciplinary team in the difficult decision-making process and communication with family members from the earliest stages of poor-grade aSAH. Further prospective studies are warranted.
即使采用积极治疗,低级别动脉瘤性蛛网膜下腔出血(aSAH)患者的管理仍面临不良预后的负担。本研究的目的是调查影响低级别aSAH患者30天死亡率的危险因素。
我们对2010年12月至2020年12月在本机构治疗的低级别aSAH患者(世界神经外科协会联合会,WFNS,IV级和V级)的前瞻性收集数据库进行了回顾性分析。对于所有变量,分析了频率分布的百分比。列联表(卡方检验)用于在单变量分析中评估分类变量与结局之间的关联。多变量分析采用多元逻辑回归方法来估计30天死亡率的比值比(OR)。
共纳入149例患者,其中32%为WFNS 4级,68%为WFNS 5级。总体1个月死亡率为21%。在单变量分析中,发现五个变量与死亡可能性相关,包括脑室内出血(IVH≥50 mL,P = 0.005)、脑室内和脑实质内出血总量(IVH + ICH≥90 mL,P = 0.019)、IVH比例(IVH比例≥40%,P = 0.003)、后循环动脉瘤(P = 0.019)、初始CT扫描血管造影上的斑点征(P = 0.015)。然而,在进行多变量分析时,只有IVH比例(P = 0.005;OR 3.97)、后循环动脉瘤(P = 0.008;OR 4.05)和斑点征(P = 0.022;OR 6.87)被证明是30天死亡率的独立预测因素。
尽管进行了最大程度的治疗,低级别aSAH的死亡风险仍然相当大。尽管回顾性研究存在局限性,但我们的报告强调了一些神经放射学特征,在紧急情况下,结合主要的临床和既往参数,可能有助于多学科团队在低级别aSAH的早期阶段进行艰难的决策过程并与家属沟通。有必要进行进一步的前瞻性研究。