Tan Daniel J, Plasek Joseph M, Hou Peter C, Baron Rebecca M, Atkinson Benjamin J, Zhou Li
Department of Biomedical Informatics, Harvard Medical School, Boston, MA.
Division of General Internal Medicine and Primary Care, Department of Medicine, Brigham and Women's Hospital, Harvard Medical School, Boston, MA.
Crit Care Explor. 2024 Mar 5;6(3):e1043. doi: 10.1097/CCE.0000000000001043. eCollection 2024 Mar.
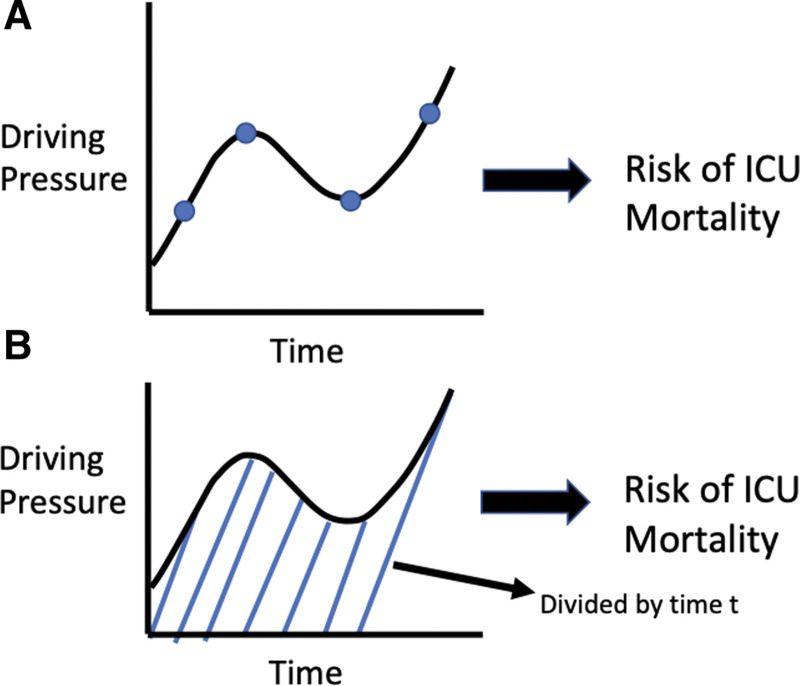
COVID-19-related acute respiratory distress syndrome (ARDS) is associated with high mortality and often necessitates invasive mechanical ventilation (IMV). Previous studies on non-COVID-19 ARDS have shown driving pressure to be robustly associated with ICU mortality; however, those studies relied on "static" driving pressure measured periodically and manually. As "continuous" automatically monitored driving pressure is becoming increasingly available and reliable with more advanced mechanical ventilators, we aimed to examine the effect of this "dynamic" driving pressure in COVID-19 ARDS throughout the entire ventilation period.
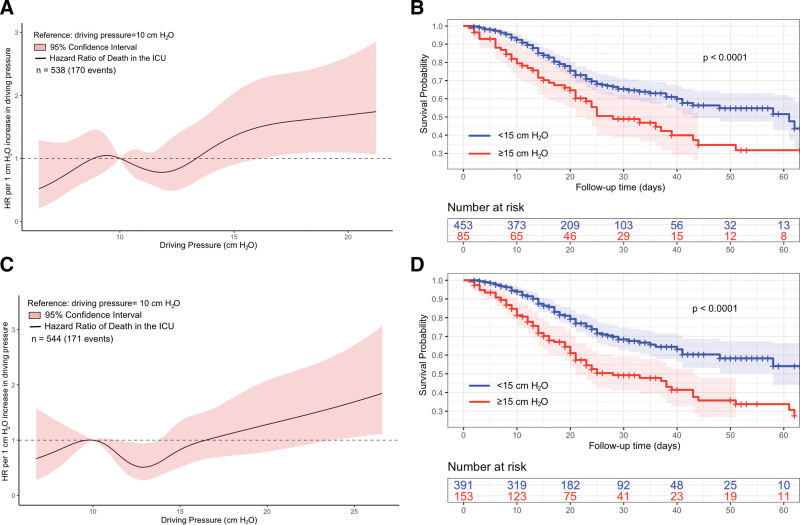
This retrospective, observational study cohort study evaluates the association between driving pressure and ICU mortality in patients with concurrent COVID-19 and ARDS using multivariate joint modeling. The study cohort ( = 544) included all adult patients (≥ 18 yr) with COVID-19 ARDS between March 1, 2020, and April 30, 2021, on volume-control mode IMV for 12 hours or more in a Mass General Brigham, Boston, MA ICU.
Of 544 included patients, 171 (31.4%) died in the ICU. Increased dynamic ΔP was associated with increased risk in the hazard of ICU mortality (hazard ratio [HR] 1.035; 95% credible interval, 1.004-1.069) after adjusting for other relevant dynamic respiratory biomarkers. A significant increase in risk in the hazard of death was found for every hour of exposure to high intensities of driving pressure (≥ 15 cm HO) (HR 1.002; 95% credible interval 1.001-1.003).
Limiting patients' exposure to high intensities of driving pressure even while under lung-protective ventilation may represent a critical step in improving ICU survival in patients with COVID-19 ARDS. Time-series IMV data could be leveraged to enhance real-time monitoring and decision support to optimize ventilation strategies at the bedside.
新型冠状病毒肺炎(COVID-19)相关的急性呼吸窘迫综合征(ARDS)死亡率高,常需有创机械通气(IMV)。既往针对非COVID-19 ARDS的研究表明,驱动压与重症监护病房(ICU)死亡率密切相关;然而,这些研究依赖于定期手动测量的“静态”驱动压。随着更先进的机械通气设备使“连续”自动监测的驱动压越来越容易获得且可靠,我们旨在研究这种“动态”驱动压在整个通气期间对COVID-19 ARDS患者的影响。
设计、设置及参与者:这项回顾性观察性队列研究采用多变量联合模型评估同时患有COVID-19和ARDS的患者中驱动压与ICU死亡率之间的关联。研究队列(n = 544)包括2020年3月1日至2021年4月30日期间在马萨诸塞州波士顿市布莱根妇女医院重症监护病房接受容量控制模式IMV且时长达12小时或更长时间的所有成年(≥18岁)COVID-19 ARDS患者。
在纳入研究的544例患者中,171例(31.4%)在ICU死亡。在调整其他相关动态呼吸生物标志物后,动态驱动压增量(ΔP)升高与ICU死亡风险增加相关(风险比[HR] 1.035;95%可信区间,1.004 - 1.069)。每暴露于高强度驱动压(≥15 cm H₂O)1小时,死亡风险显著增加(HR 1.002;95%可信区间1.001 - 1.003)。
即使在肺保护性通气情况下,限制患者暴露于高强度驱动压可能是提高COVID-19 ARDS患者ICU生存率的关键一步。可利用时间序列IMV数据加强实时监测和决策支持,以优化床边通气策略。