J Orthop Traumatol. 2024 Mar 7;25(1):13. doi: 10.1186/s10195-024-00746-6.
The incidence of all periprosthetic fractures (PPF), which require complex surgical treatment associated with high morbidity and mortality, is predicted to increase. The evolving surgical management has created a knowledge gap regarding its impact on immediate outcomes. This study aimed to describe current management strategies for PPF and their repercussions for in-hospital outcomes as well as to evaluate their implications for the community.
PIPPAS (Peri-Implant PeriProsthetic Survival Analysis) was a prospective multicentre observational study of 1387 PPF performed during 2021. Descriptive statistics summarized the epidemiology, fracture characteristics, management, and immediate outcomes. A mixed-effects logistic regression model was employed to evaluate potential predictors of in-hospital mortality, complications, discharge status, and weight-bearing restrictions.
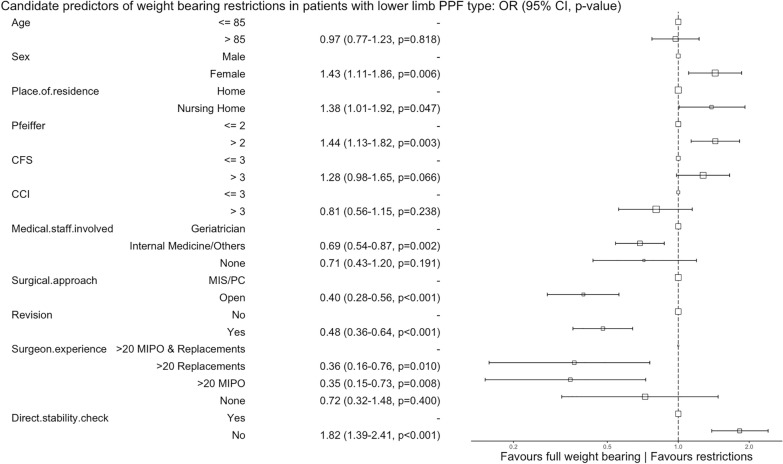
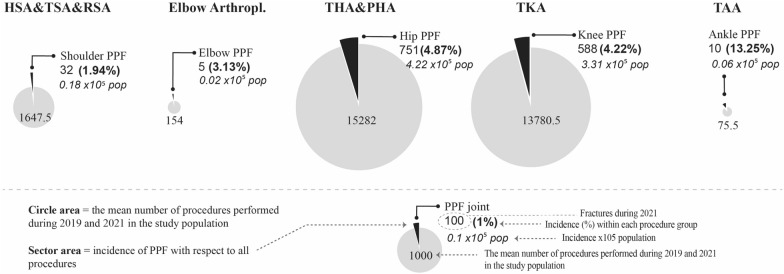
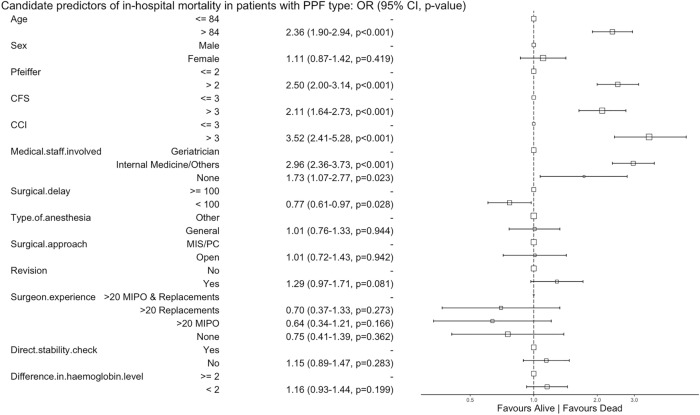
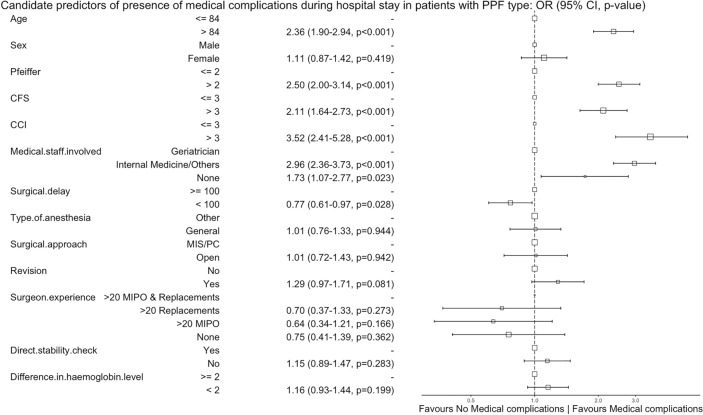
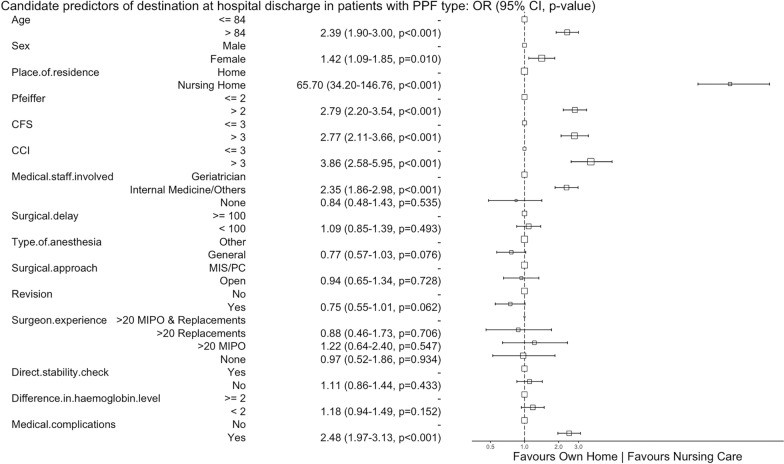
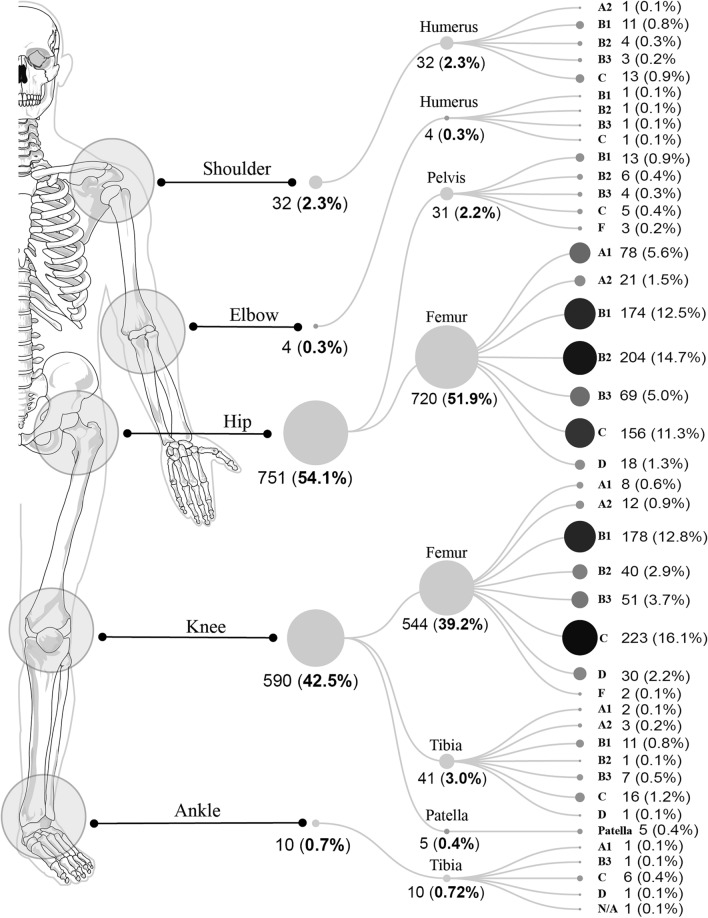
The study encompassed 32 (2.3%) shoulder, 4 (0.3%) elbow, 751 (54.1%) hip, 590 (42.5%) knee, and 10 (0.7%) ankle PPF. Patients were older (median 84 years, IQR 77-89), frail [median clinical frailty scale (CFS) 5, IQR 3-6], presented at least one comorbidity [median Charlson comorbidity index (CCI) 5, IQR 4-7], were community dwelling (81.8%), and had outdoor ambulation ability (65.6%). Femoral knee PPF were most frequently associated with uncemented femoral components, while femoral hip PPF occurred equally in cemented and uncemented stems. Patients were managed surgically (82%), with co-management (73.9%), through open approaches (85.9%) after almost 4 days (IQR, 51.9-153.6 h), with prosthesis revision performed in 33.8% of femoral hip PPF and 6.5% of femoral knee PPF. For half of the patients, the discharge instructions mandated weight-bearing restrictions. In-hospital mortality rates were 5.2% for all PPF and 6.2% for femoral hip PPF. Frailty, age > 84 years, mild cognitive impairment, CFS > 3, CCI > 3, and non-geriatric involvement were candidate predictors for in-hospital mortality, medical complications, and discharge to a nursing care facility. Management involving revision arthroplasty by experienced surgeons favoured full weight-bearing, while an open surgical approach favoured weight-bearing restrictions.
Current arthroplasty fixation check and revision rates deviate from established guidelines, yet full weight-bearing is favoured. A surgical delay of over 100 h and a lack of geriatric co-management were related to in-hospital mortality and medical complications. This study recommends judicious hypoaggressive approaches. Addressing complications and individualizing the surgical strategy can lead to enhanced functional outcomes, alleviating the economic and social burdens upon hospital discharge. Level of Evidence Level IV case series.
registered at ClinicalTrials.gov (NCT04663893), protocol ID: PI 20-2041.
需要复杂手术治疗且具有较高发病率和死亡率的全髋关节假体周围骨折(PPF)的发病率预计将会增加。不断发展的手术治疗方法在其对即时结果的影响方面存在知识空白。本研究旨在描述 PPF 的当前治疗策略及其对住院期间结果的影响,并评估其对社区的影响。
PPIPAS(假体周围假体生存分析)是一项针对 2021 年期间进行的 1387 例 PPF 的前瞻性多中心观察性研究。描述性统计数据总结了流行病学、骨折特征、管理和即时结果。采用混合效应逻辑回归模型评估住院期间死亡率、并发症、出院状态和负重限制的潜在预测因素。
研究包括 32 例(2.3%)肩部、4 例(0.3%)肘部、751 例(54.1%)髋部、590 例(42.5%)膝关节和 10 例(0.7%)踝关节 PPF。患者年龄较大(中位数 84 岁,IQR 77-89),虚弱[中位数临床虚弱量表(CFS)5,IQR 3-6],存在至少一种合并症[中位数 Charlson 合并症指数(CCI)5,IQR 4-7],居住在社区(81.8%),具有户外活动能力(65.6%)。股骨膝关节 PPF 最常与非骨水泥股骨组件相关,而股骨髋关节 PPF 则在骨水泥和非骨水泥柄中发生率相等。患者接受手术治疗(82%),联合管理(73.9%),通过开放入路(85.9%)进行治疗,几乎需要 4 天(IQR,51.9-153.6 h)后进行假体翻修,33.8%的股骨髋关节 PPF 和 6.5%的股骨膝关节 PPF 进行了翻修。对于一半的患者,出院医嘱要求限制负重。所有 PPF 的住院死亡率为 5.2%,股骨髋关节 PPF 的住院死亡率为 6.2%。虚弱、年龄>84 岁、轻度认知障碍、CFS>3、CCI>3 和非老年患者是住院期间死亡率、医疗并发症和出院至护理院的候选预测因素。由经验丰富的外科医生进行的翻修关节置换术管理有利于完全负重,而开放手术方法有利于负重限制。
当前的关节置换固定检查和翻修率与既定指南不符,但仍倾向于完全负重。手术延迟超过 100 h 和缺乏老年患者的联合管理与住院期间死亡率和医疗并发症相关。本研究建议采用谨慎的低攻击性方法。处理并发症和个体化手术策略可以改善功能结局,减轻出院后对医院的经济和社会负担。研究类型:病例系列研究。
IV 级临床试验。
ClinicalTrials.gov 注册(NCT04663893),方案 ID:PI 20-2041。