Berenguer Juan, Aldámiz-Echevarría Teresa, Hontañón Víctor, Fanciulli Chiara, Quereda Carmen, Busca Carmen, Domínguez Lourdes, Hernández Cristina, Vergas Jorge, Gaspar Gabriel, García-Fraile Lucio J, Díez Cristina, De Miguel Marta, Bellón José M, Bañares Rafael, González-García Juan
Infectious Diseases/Clinical Microbiology, Hospital General Universitario Gregorio Marañón, Madrid, Spain.
Instituto de Investigación Sanitaria Gregorio Marañón (IiSGM), Madrid, Spain.
Hepatology. 2025 Jan 1;81(1):238-253. doi: 10.1097/HEP.0000000000000838. Epub 2024 Mar 7.
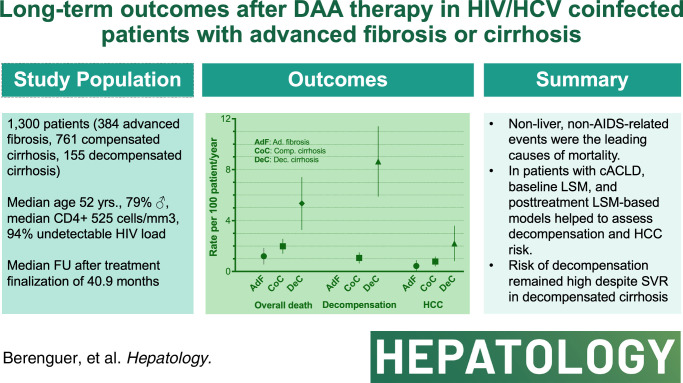
We assessed long-term clinical outcomes and prognostic factors for liver disease progression after sustained viral response with direct-acting antivirals in patients coinfected with HIV/HCV with advanced fibrosis or cirrhosis.
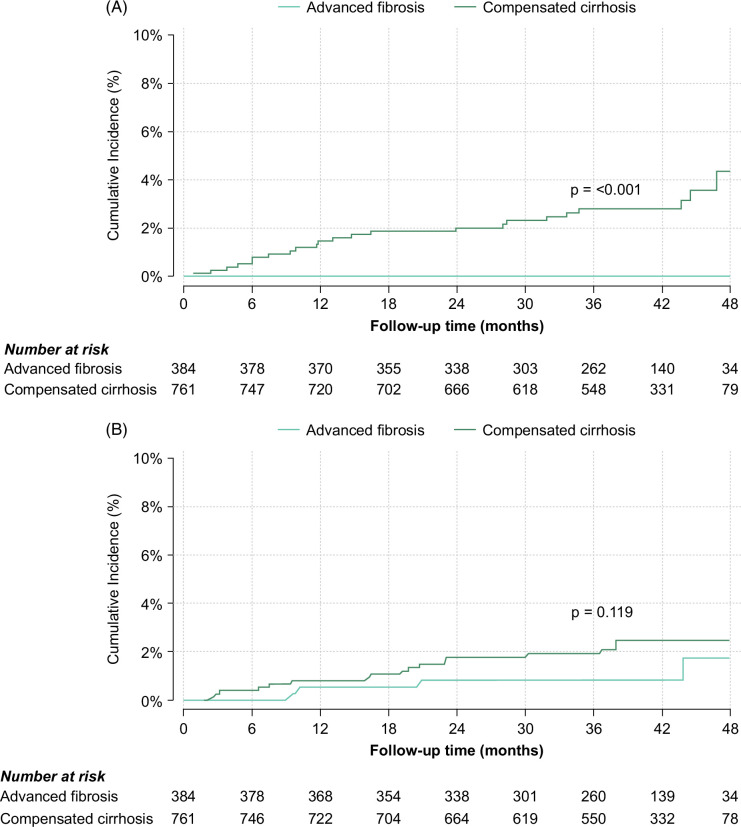
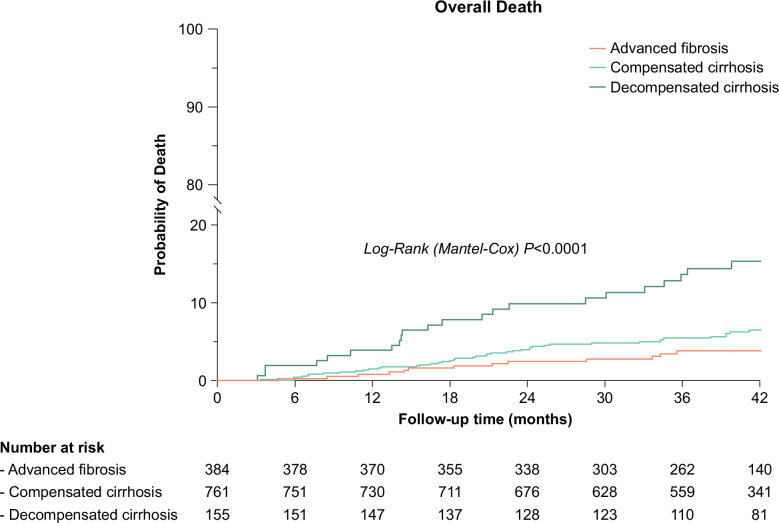
A total of 1300 patients who achieved sustained viral response with direct-acting antivirals from 2014 to 2017 in Spain were included: 1145 with compensated advanced chronic liver disease (384 advanced fibrosis and 761 compensated cirrhosis) and 155 with decompensated cirrhosis. The median follow-up was 40.9 months. Overall, 85 deaths occurred, 61 due to non-liver non-AIDS-related causes that were the leading cause of death across all stages of liver disease. The incidence (95% CI) of decompensation per 100 person-years (py) was 0 in patients with advanced fibrosis, 1.01 (0.68-1.51) in patients with compensated cirrhosis, and 8.35 (6.05-11.53) in patients with decompensated cirrhosis. The incidence (95% CI) of HCC per 100 py was 0.34 (0.13-0.91) in patients with advanced fibrosis, 0.73 (0.45-1.18) in patients with compensated cirrhosis, and 1.92 (1.00-3.70) per 100 py in patients with decompensated cirrhosis. Prognostic factors for decompensation in patients with compensated advanced chronic liver disease included serum albumin, liver stiffness measurement (LSM), and fibrosis 4. In this population, LSM and LSM-based posttreatment risk stratification models showed their predictive ability for decompensation and HCC.
Non-liver non-AIDS-related events were the leading causes of morbidity and mortality after direct-acting antiviral cure among coinfected patients with advanced fibrosis/cirrhosis. Among those with compensated advanced chronic liver disease, baseline LSM and posttreatment LSM-based models helped to assess decompensation and HCC risk.
我们评估了在合并晚期纤维化或肝硬化的HIV/HCV合并感染患者中,使用直接作用抗病毒药物实现持续病毒学应答后肝病进展的长期临床结局及预后因素。
纳入了2014年至2017年在西班牙使用直接作用抗病毒药物实现持续病毒学应答的1300例患者:1145例为代偿期晚期慢性肝病(384例为晚期纤维化,761例为代偿期肝硬化),155例为失代偿期肝硬化。中位随访时间为40.9个月。总体上,发生了85例死亡,其中61例死于非肝脏非艾滋病相关原因,这是所有肝病阶段的主要死亡原因。每100人年(py)失代偿的发生率(95%CI)在晚期纤维化患者中为0,在代偿期肝硬化患者中为1.01(0.68 - 1.51),在失代偿期肝硬化患者中为8.35(6.05 - 11.53)。每100 py肝细胞癌(HCC)的发生率(95%CI)在晚期纤维化患者中为0.34(0.13 - 0.91),在代偿期肝硬化患者中为0.73(0.45 - 1.18),在失代偿期肝硬化患者中为每100 py 1.92(1.00 - 3.70)。代偿期晚期慢性肝病患者失代偿的预后因素包括血清白蛋白、肝脏硬度测量(LSM)和纤维化4项指标。在该人群中,LSM及基于LSM的治疗后风险分层模型显示了其对失代偿和HCC的预测能力。
在合并晚期纤维化/肝硬化的合并感染患者中,直接作用抗病毒药物治愈后,非肝脏非艾滋病相关事件是发病和死亡的主要原因。在代偿期晚期慢性肝病患者中,基线LSM及基于治疗后LSM的模型有助于评估失代偿和HCC风险。