Lu Hui-Fei, Li Jing-Jing, Zhu De-Bin, Mao Li-Qi, Xu Li-Fen, Yu Jing, Yao Lin-Hua
Department of Gastroenterology, the First People's Hospital of Huzhou, Huzhou 313000, Zhejiang Province, China.
World J Gastrointest Surg. 2024 Feb 27;16(2):601-608. doi: 10.4240/wjgs.v16.i2.601.
Gastric stromal tumors, originating from mesenchymal tissues, are one of the most common tumors of the digestive tract. For stromal tumors originating from the muscularis propria, compared with conventional endoscopic submucosal dissection (ESD), endoscopic full-thickness resection (EFTR) can remove deep lesions and digestive tract wall tumors completely. However, this technique has major limitations such as perforation, postoperative bleeding, and post-polypectomy syndrome. Herein, we report a case of postoperative serous surface bleeding which formed an encapsulated hemoperitoneum in a patient with gastric stromal tumor that was treated with exposed EFTR. Feasible treatment options to address this complication are described.
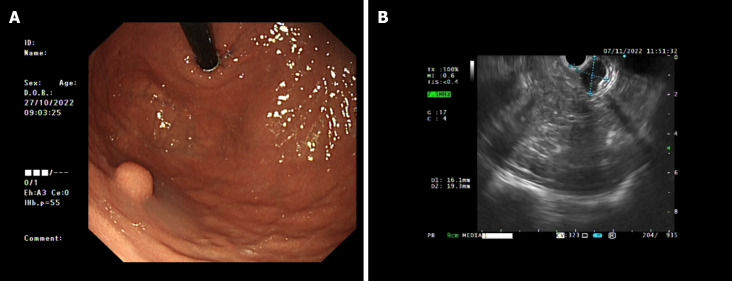
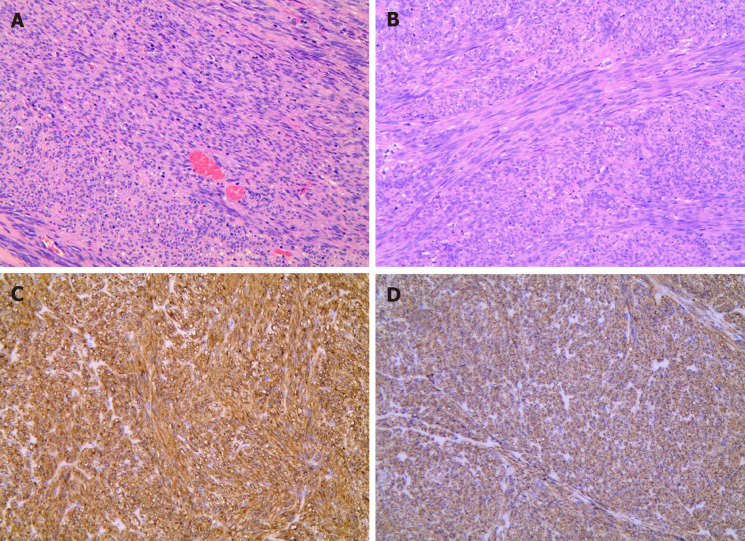
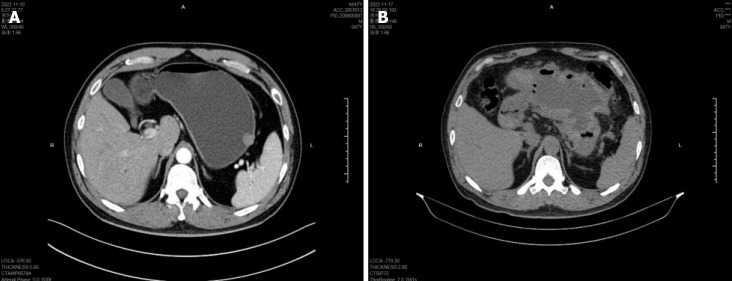
A 47-year-old male patient had a hemispherical protrusion found during gastric endoscopic ultrasonography, located at the upper gastric curvature adjacent to the stomach fundus, with a smooth surface mucosa and poor mobility. The lesion was 19.3 mm × 16.1 mm in size and originated from the fourth ultrasound layer. Computed tomography (CT) revealed no significant evidence of lymph node enlargement or distant metastasis. Using conventional ESD technology for mucosal pre-resection, exposed EFTR was performed to resect the intact tumor in order to achieve a definitive histopathological diagnosis. Based on its morphology and immunohistochemical expression of CD117 and DOG-1, the lesion was proven to be consistent with a gastric stromal tumor. Six days after exposed EFTR, CT showed a large amount of encapsulated fluid and gas accumulation around the stomach. In addition, gastroscopy suggested intracavitary bleeding and abdominal puncture drainage indicated serosal bleeding. Based on these findings, the patient was diagnosed with serosal bleeding resulting in encapsulated abdominal hemorrhage after exposed EFTR for a gastric stromal tumor. The patient received combined treatments, such as hemostasis under gastroscopy, gastrointestinal decompression, and abdominal drainage. All examinations were normal within six months of follow-up.
This patient developed serous surface bleeding in the gastric cavity following exposed EFTR. Serosal bleeding resulting in an encapsulated hemoperitoneum is rare in clinical practice. The combined treatment may replace certain surgical techniques.
胃间质瘤起源于间叶组织,是消化道最常见的肿瘤之一。对于起源于固有肌层的间质瘤,与传统内镜黏膜下剥离术(ESD)相比,内镜全层切除术(EFTR)能够完整切除深部病变及消化道壁肿瘤。然而,该技术存在诸如穿孔、术后出血及息肉切除术后综合征等主要局限性。在此,我们报告1例胃间质瘤患者在接受暴露式EFTR治疗后发生术后浆膜面出血并形成包裹性血腹的病例,并描述了针对该并发症的可行治疗方案。
1例47岁男性患者在胃镜超声检查时发现胃体上部大弯侧近胃底处有一半球形隆起,表面黏膜光滑,活动度差。病变大小为19.3 mm×16.1 mm,起源于超声第四层。计算机断层扫描(CT)未发现明显的淋巴结肿大或远处转移迹象。采用传统ESD技术进行黏膜预切除,然后行暴露式EFTR完整切除肿瘤以获得确切的组织病理学诊断。根据其形态及CD117和DOG-1的免疫组化表达,证实该病变符合胃间质瘤。暴露式EFTR术后6天,CT显示胃周有大量包裹性液体和气体积聚。此外,胃镜提示腔内出血,腹腔穿刺引流提示浆膜出血。基于这些发现,该患者被诊断为胃间质瘤暴露式EFTR术后浆膜出血导致包裹性腹腔内出血。患者接受了胃镜下止血、胃肠减压及腹腔引流等综合治疗。随访6个月内所有检查均正常。
该患者在暴露式EFTR术后出现胃腔内浆膜面出血。浆膜出血导致包裹性血腹在临床实践中较为罕见。综合治疗可能替代某些外科手术技术。