Zhang Hong-Ying, He Chen-Cong
Department of Gastroenterology, Jinhua People's Hospital, Jinhua 321000, Zhejiang Province, China.
Department of General Medicine, Jinhua Guangfu Hospital, Jinhua 321001, Zhejiang Province, China.
World J Gastrointest Surg. 2024 Feb 27;16(2):609-615. doi: 10.4240/wjgs.v16.i2.609.
Infected acute necrotic collection (ANC) is a fatal complication of acute pancreatitis with substantial morbidity and mortality. Drainage plays an exceedingly important role as the first step in invasive intervention for infected necrosis; however, there is great controversy about the optimal drainage time, and better treatment should be explored.
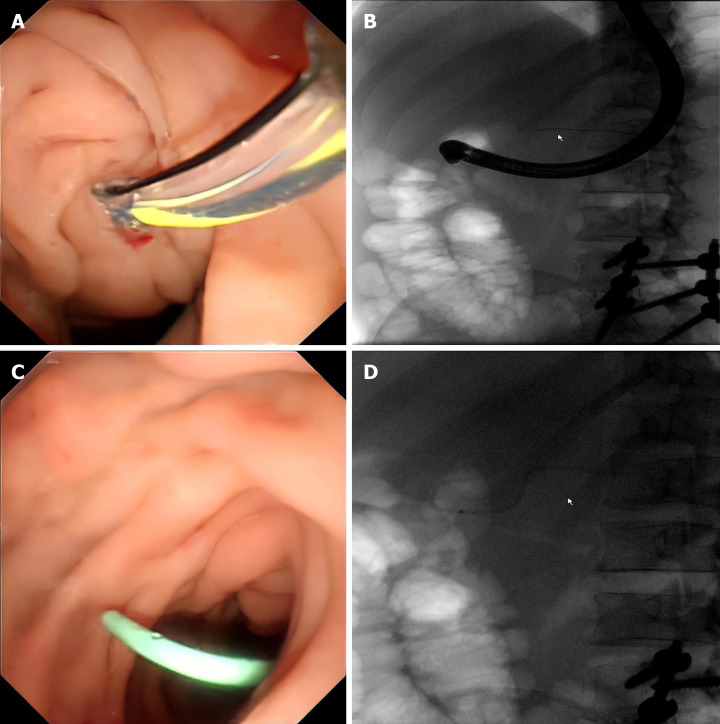
We report the case of a 43-year-old man who was admitted to the hospital with severe intake reduction due to early satiety 2 wk after treatment for acute pancreatitis; conservative treatment was ineffective, and a pancreatic pseudocyst was suspected on contrast-enhanced computed tomography (CT). Endoscopic ultrasonography (EUS) suggested hyperechoic necrotic tissue within the cyst cavity. The wall was not completely mature, and the culture of the puncture fluid was positive for A-haemolytic Streptococcus. Thus, the final diagnosis of ANC infection was made. The necrotic collection was not walled off and contained many solid components; therefore, the patient underwent EUS-guided aspiration and lavage. Two weeks after the collection was completely encapsulated, pancreatic duct stent drainage endoscopic retrograde cholangiopancreatography (ERCP) was performed, and the patient was subsequently successfully discharged. On repeat CT, the pancreatic cysts had almost disappeared during the 6-month follow-up period after surgery.
Early EUS-guided aspiration and lavage combined with late ERCP catheter drainage may be effective methods for intervention in infected ANCs.
感染性急性坏死性积液(ANC)是急性胰腺炎的一种致命并发症,具有较高的发病率和死亡率。引流作为感染性坏死侵入性干预的第一步起着极其重要的作用;然而,关于最佳引流时间存在很大争议,应探索更好的治疗方法。
我们报告一例43岁男性患者,在急性胰腺炎治疗2周后因早饱导致严重进食减少入院;保守治疗无效,对比增强计算机断层扫描(CT)怀疑有胰腺假性囊肿。内镜超声检查(EUS)提示囊肿腔内有高回声坏死组织。囊壁未完全成熟,穿刺液培养A溶血性链球菌阳性。因此,最终诊断为ANC感染。坏死性积液未形成包裹且含有许多实性成分;因此,患者接受了EUS引导下的抽吸和灌洗。在积液完全包裹两周后,进行了胰管支架引流及内镜逆行胰胆管造影(ERCP),患者随后成功出院。术后6个月随访期间复查CT显示胰腺囊肿几乎消失。
早期EUS引导下抽吸和灌洗联合后期ERCP导管引流可能是干预感染性ANC的有效方法。