Hao Sicheng, Dempsey Katelyn, Matos João, Cox Christopher E, Rotemberg Veronica, Gichoya Judy W, Kibbe Warren, Hong Chuan, Wong Ian
Duke University, Department of Medicine, Division of Pulmonary, Allergy, and Critical Care Medicine, Durham, NC, USA.
Memorial-Sloan Kettering, Dermatology Service, New York, NY, USA.
medRxiv. 2024 Feb 27:2024.02.24.24303291. doi: 10.1101/2024.02.24.24303291.
Pulse oximetry, a ubiquitous vital sign in modern medicine, has inequitable accuracy that disproportionately affects Black and Hispanic patients, with associated increases in mortality, organ dysfunction, and oxygen therapy. Although the root cause of these clinical performance discrepancies is believed to be skin tone, previous retrospective studies used self-reported race or ethnicity as a surrogate for skin tone.
To determine the utility of objectively measured skin tone in explaining pulse oximetry discrepancies.
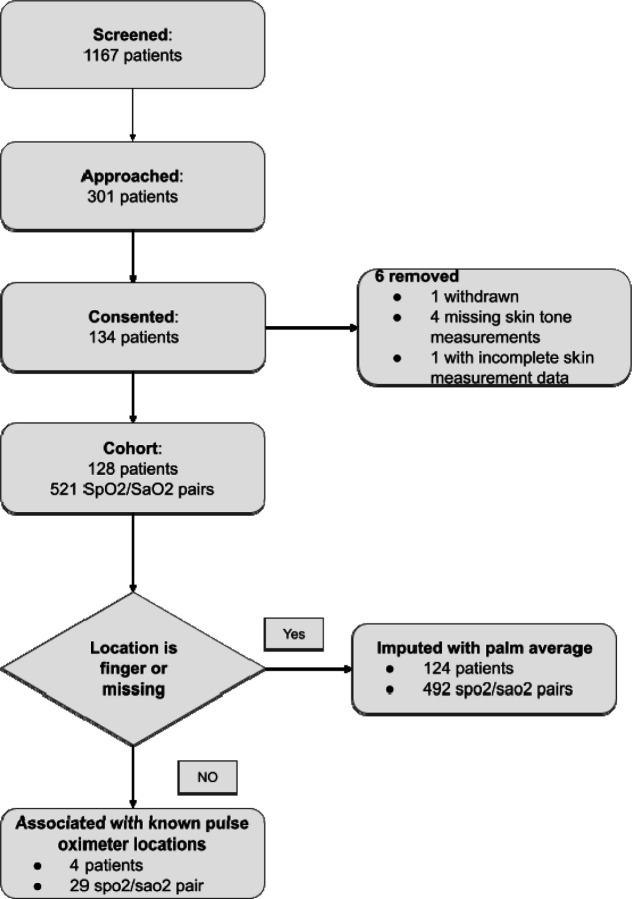
Admitted hospital patients at Duke University Hospital were eligible for this prospective cohort study if they had pulse oximetry recorded up to 5 minutes prior to arterial blood gas (ABG) measurements. Skin tone was measured across sixteen body locations using administered visual scales (Fitzpatrick Skin Type, Monk Skin Tone, and Von Luschan), reflectance colorimetry (Delfin SkinColorCatch [L*, individual typology angle {ITA}, Melanin Index {MI}]), and reflectance spectrophotometry (Konica Minolta CM-700D [L*], Variable Spectro 1 [L*]).
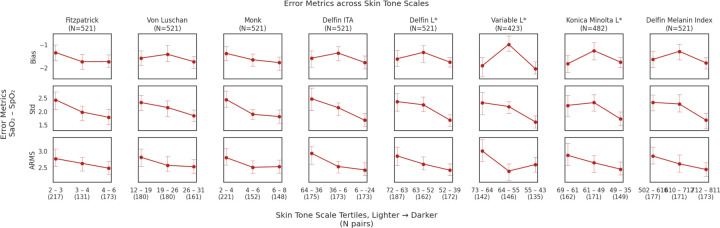
Mean directional bias, variability of bias, and accuracy root mean square (A), comparing pulse oximetry and ABG measurements. Linear mixed-effects models were fitted to estimate mean directional bias while accounting for clinical confounders.
128 patients (57 Black, 56 White) with 521 ABG-pulse oximetry pairs were recruited, none with hidden hypoxemia. Skin tone data was prospectively collected using 6 measurement methods, generating 8 measurements. The collected skin tone measurements were shown to yield differences among each other and overlap with self-reported racial groups, suggesting that skin tone could potentially provide information beyond self-reported race. Among the eight skin tone measurements in this study, and compared to self-reported race, the Monk Scale had the best relationship with differences in pulse oximetry bias (point estimate: -2.40%; 95% CI: -4.32%, -0.48%; =0.01) when comparing patients with lighter and dark skin tones.
We found clinical performance differences in pulse oximetry, especially in darker skin tones. Additional studies are needed to determine the relative contributions of skin tone measures and other potential factors on pulse oximetry discrepancies.
脉搏血氧饱和度测定法是现代医学中一种普遍使用的生命体征,但存在不公平的准确性问题,对黑人和西班牙裔患者的影响尤为严重,这与死亡率、器官功能障碍和氧疗的增加有关。尽管这些临床表现差异的根本原因被认为是肤色,但以往的回顾性研究使用自我报告的种族或族裔作为肤色的替代指标。
确定客观测量的肤色在解释脉搏血氧饱和度差异方面的作用。
设计、地点和参与者:如果杜克大学医院的住院患者在进行动脉血气(ABG)测量前5分钟内记录了脉搏血氧饱和度,则符合这项前瞻性队列研究的条件。使用视觉量表(菲茨帕特里克皮肤类型、蒙克肤色和冯·卢尚)、反射比色法(德尔芬皮肤颜色捕捉仪[L*、个体类型角度{ITA}、黑色素指数{MI}])和反射分光光度法(柯尼卡美能达CM - 700D[L*]、可变光谱仪1[L*])在16个身体部位测量肤色。
比较脉搏血氧饱和度测定法和ABG测量的平均方向偏差、偏差的变异性和准确性均方根(A)。拟合线性混合效应模型以估计平均方向偏差,同时考虑临床混杂因素。
招募了128名患者(57名黑人、56名白人),有521对ABG - 脉搏血氧饱和度测定数据,均无隐匿性低氧血症。使用6种测量方法前瞻性收集肤色数据,得出8项测量结果。所收集的肤色测量结果显示彼此之间存在差异,且与自我报告的种族群体有重叠,这表明肤色可能提供超出自我报告种族的信息。在本研究的8项肤色测量中,与自我报告的种族相比,在比较肤色较浅和较深的患者时,蒙克量表与脉搏血氧饱和度偏差差异的关系最佳(点估计:-2.40%;95%置信区间:-4.32%,-0.48%;P = 0.01)。
我们发现脉搏血氧饱和度测定法存在临床性能差异,尤其是在肤色较深的患者中。需要进一步研究以确定肤色测量和其他潜在因素对脉搏血氧饱和度差异的相对贡献。