Knight Cancer Institute, Oregon Health and Science University, Portland, OR, USA.
Department of Radiology, Massachusetts General Hospital, Boston, MA, USA.
J Cachexia Sarcopenia Muscle. 2024 Jun;15(3):1030-1040. doi: 10.1002/jcsm.13426. Epub 2024 Mar 11.
This post hoc, pooled analysis examined the relationship between different weight gain categories and overall survival (OS) in patients with non-small cell lung cancer (NSCLC) receiving first-line platinum-based chemotherapy.
Data were pooled from the control arms of three phase III clinical studies (NCT00596830, NCT00254891, and NCT00254904), and the maximum weight gain in the first 3 months from treatment initiation was categorised as >0%, >2.5%, and >5.0%. Cox proportional hazard modelling of OS was used to estimate hazard ratios (HRs) for each category, including baseline covariates, time to weight gain, and time to confirmed objective response (RECIST Version 1.0).
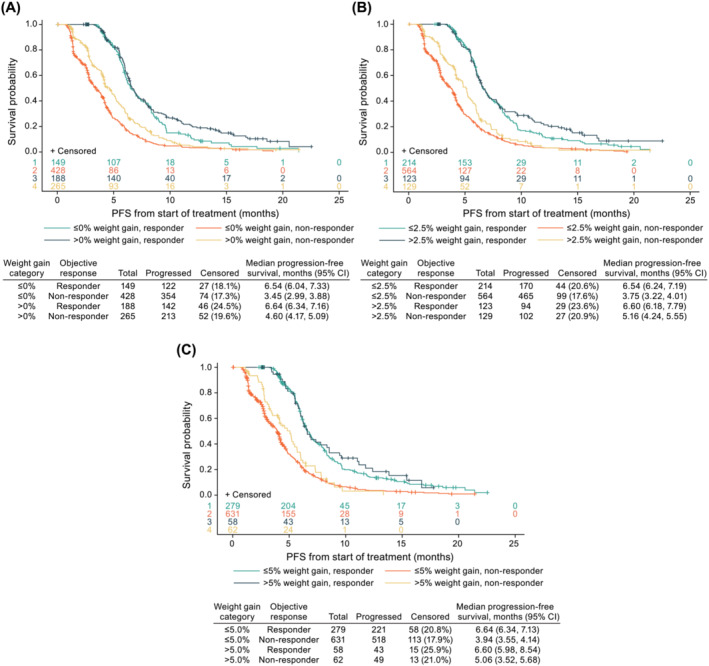
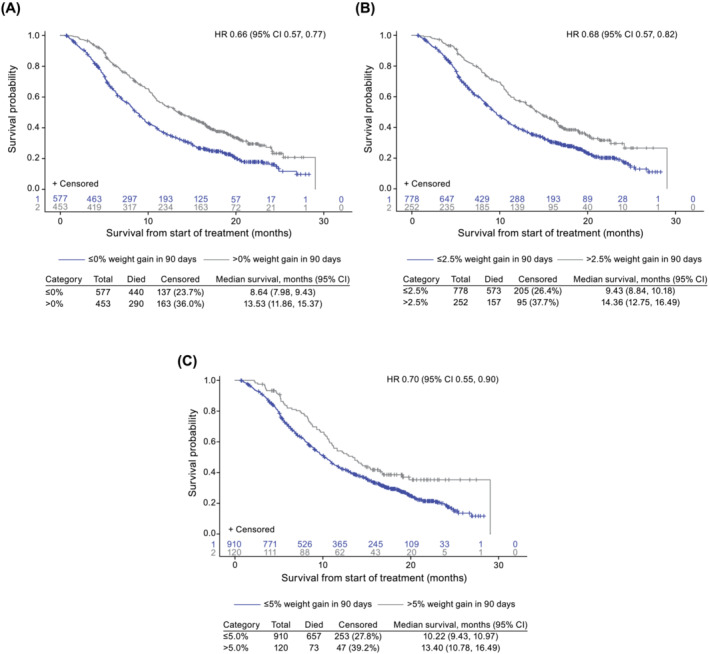
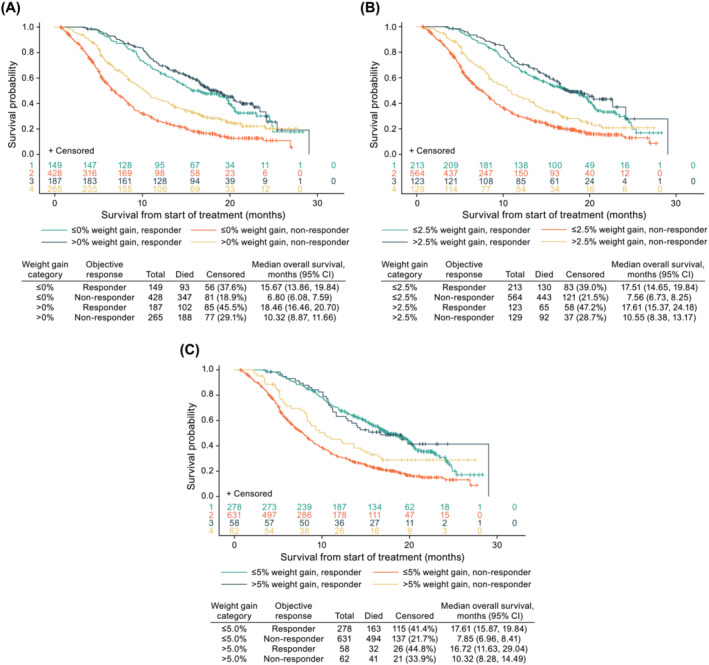
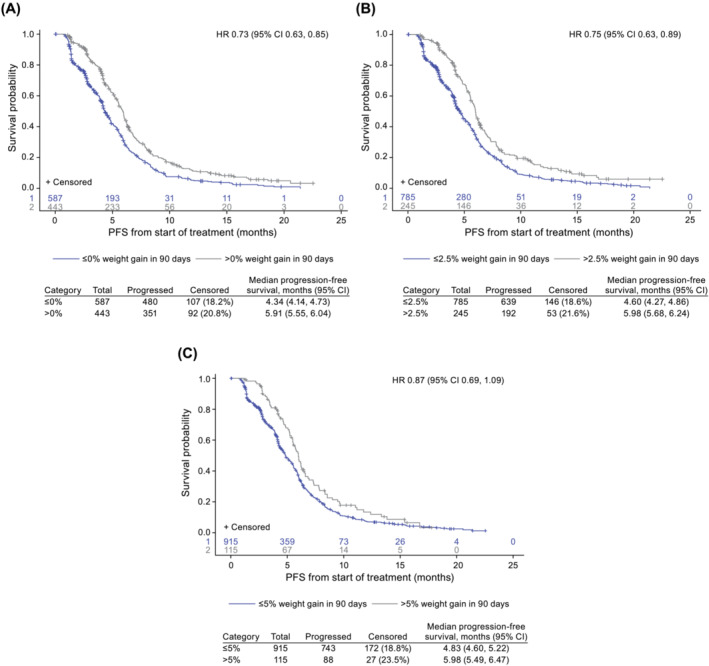
Of 1030 patients with advanced NSCLC (IIIB 11.5% and IV 88.5%), 453 (44.0%), 252 (24.5%), and 120 (11.7%) experienced weight gain from baseline of >0%, >2.5%, and >5.0%, respectively. The median time to weight gain was 23 (>0%), 43 (>2.5%), and 45 (>5.0%) days. After adjusting for a time-dependent confirmed objective response, the risk of death was reduced for patients with any weight gain (>0% vs. ≤0% [HR 0.71; 95% confidence interval-CI 0.61, 0.82], >2.5% vs. ≤2.5% [HR 0.76; 95% CI 0.64, 0.91] and >5.0% vs. ≤5.0% [HR 0.77; 95% CI 0.60, 0.99]). The median OS was 13.5 versus 8.6 months (weight gain >0% vs. ≤0%), 14.4 versus 9.4 months (weight gain >2.5% vs. ≤2.5%), and 13.4 versus 10.2 months (weight gain >5.0% vs. ≤5.0%).
Weight gain during treatment was associated with a reduced risk of death, independent of tumour response. The survival benefit was comparable for weight gain >0%, >2.5%, and >5.0%, suggesting that any weight gain may be an early predictor of survival with implications for the design of interventional cancer cachexia studies.
本事后分析研究了一线含铂化疗的非小细胞肺癌(NSCLC)患者中不同体重增加类别与总生存期(OS)之间的关系。
数据来自三项 III 期临床试验(NCT00596830、NCT00254891 和 NCT00254904)的对照组,治疗开始后 3 个月内体重增加的最大值被分为>0%、>2.5%和>5.0%。使用 OS 的 Cox 比例风险模型来估计每个类别(包括基线协变量、体重增加时间和确认的客观缓解时间[RECIST 版本 1.0])的风险比(HR)。
1030 例晚期 NSCLC 患者(IIIB 11.5%和 IV 88.5%)中,453 例(44.0%)、252 例(24.5%)和 120 例(11.7%)从基线开始体重增加>0%、>2.5%和>5.0%。体重增加的中位时间分别为 23 天(>0%)、43 天(>2.5%)和 45 天(>5.0%)。调整确认的客观缓解后,体重增加的患者死亡风险降低(>0%与≤0%[HR 0.71;95%置信区间-CI 0.61,0.82],>2.5%与≤2.5%[HR 0.76;95% CI 0.64,0.91]和>5.0%与≤5.0%[HR 0.77;95% CI 0.60,0.99])。中位 OS 分别为 13.5 个月(体重增加>0%与≤0%)、14.4 个月(体重增加>2.5%与≤2.5%)和 13.4 个月(体重增加>5.0%与≤5.0%)。
治疗期间的体重增加与死亡风险降低相关,独立于肿瘤反应。体重增加>0%、>2.5%和>5.0%的生存获益相当,这表明任何体重增加都可能是生存的早期预测因素,对癌症恶病质干预研究的设计具有启示意义。