Samarasinghe Amali, Wong Germaine, Teixeira-Pinto Armando, Johnson David W, Hawley Carmel, Pilmore Helen, Mulley William R, Roberts Matthew A, Polkinghorne Kevan R, Boudville Neil, Davies Christopher E, Viecelli Andrea K, Ooi Esther, Larkins Nicholas G, Lok Charmaine, Lim Wai H
Department of Renal Medicine, Sir Charles Gairdner Hospital, Perth, Australia.
School of Public Health, Faculty of Medicine and Health, Sydney University, Sydney, Australia.
Clin Kidney J. 2024 Mar 7;17(3):sfad245. doi: 10.1093/ckj/sfad245. eCollection 2024 Mar.
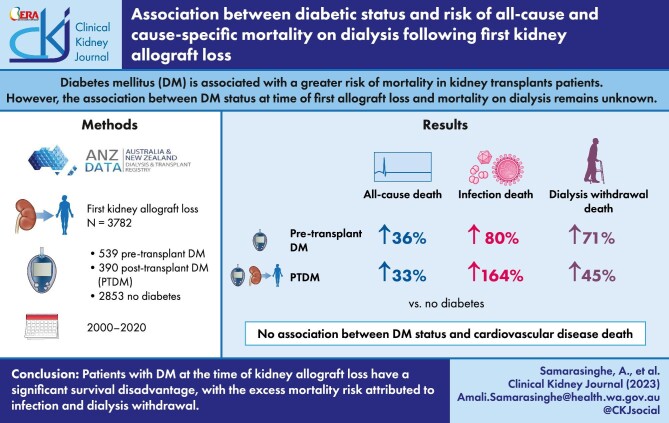
Diabetes mellitus (DM) is associated with a greater risk of mortality in kidney transplant patients, primarily driven by a greater risk of cardiovascular disease (CVD)-related mortality. However, the associations between diabetes status at time of first allograft loss and mortality on dialysis remain unknown.
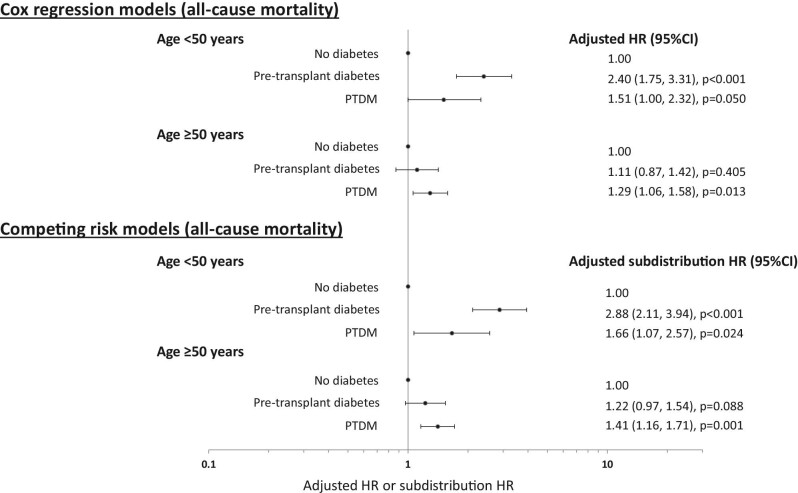
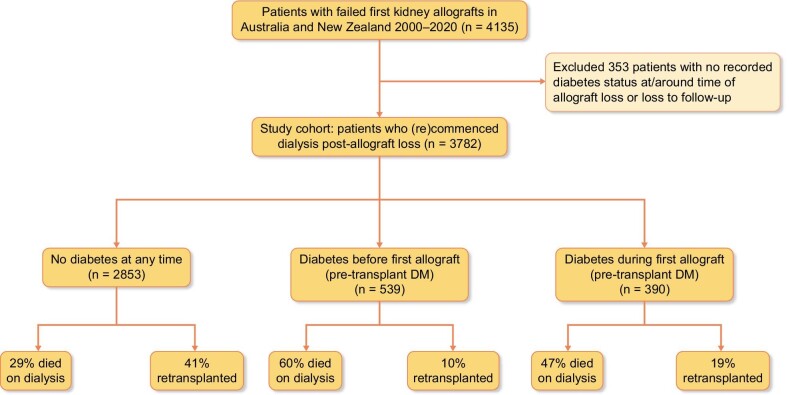
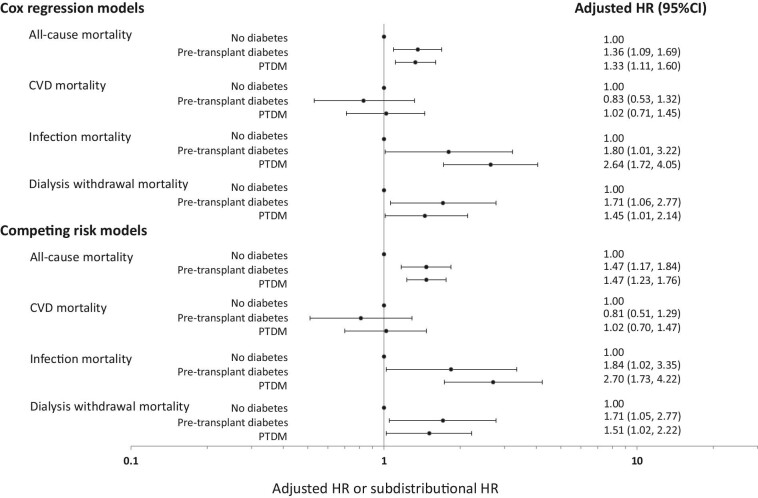
All patients with failed first kidney allografts transplanted in Australia and New Zealand between 2000 and 2020 were included. The associations between diabetes status at first allograft loss, all-cause and cause-specific mortality were examined using competing risk analyses, separating patients with diabetes into those with pre-transplant DM or post-transplant diabetes mellitus (PTDM).
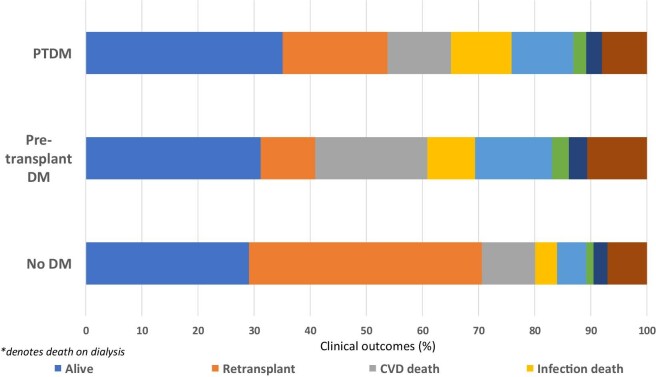
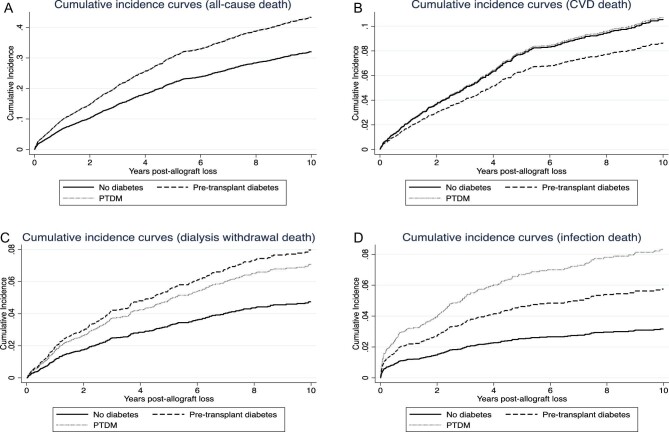
Of 3782 patients with a median (IQR) follow-up duration of 2.7 (1.1-5.4) years, 539 (14%) and 390 (10%) patients had pre-transplant DM or developed PTDM, respectively. In the follow-up period, 1336 (35%) patients died, with 424 (32%), 264 (20%) and 199 (15%) deaths attributed to CVD, dialysis withdrawal and infection, respectively. Compared to patients without DM, the adjusted subdistribution HRs (95% CI) for pre-transplant DM and PTDM for all-cause mortality on dialysis were 1.47 (1.17-1.84) and 1.47 (1.23-1.76), respectively; for CVD-related mortality were 0.81 (0.51-1.29) and 1.02 (0.70-1.47), respectively; for infection-related mortality were 1.84 (1.02-3.35) and 2.70 (1.73-4.20), respectively; and for dialysis withdrawal-related mortality were 1.71 (1.05-2.77) and 1.51 (1.02-2.22), respectively.
Patients with diabetes at the time of kidney allograft loss have a significant survival disadvantage, with the excess mortality risk attributed to infection and dialysis withdrawal.
糖尿病(DM)与肾移植患者更高的死亡风险相关,主要是由心血管疾病(CVD)相关死亡风险增加所致。然而,首次移植肾失功时的糖尿病状态与透析患者死亡率之间的关联尚不清楚。
纳入2000年至2020年间在澳大利亚和新西兰接受首次移植肾失功的所有患者。使用竞争风险分析方法,研究首次移植肾失功时的糖尿病状态与全因死亡率及特定病因死亡率之间的关联,将糖尿病患者分为移植前糖尿病患者或移植后糖尿病(PTDM)患者。
3782例患者的中位(IQR)随访时间为2.7(1.1 - 5.4)年,分别有539例(14%)和390例(10%)患者为移植前糖尿病患者或发生了PTDM。在随访期间,1336例(35%)患者死亡,分别有424例(32%)、264例(20%)和199例(15%)患者死于CVD、停止透析和感染。与非糖尿病患者相比,移植前糖尿病和PTDM患者透析时全因死亡的校正亚分布风险比(95%CI)分别为1.47(1.17 - 1.84)和1.47(1.23 - 1.76);CVD相关死亡的分别为0.81(0.51 - 1.29)和1.02(0.70 - 1.47);感染相关死亡的分别为1.84(1.02 - 3.35)和2.70(1.73 - 4.20);停止透析相关死亡的分别为1.71(1.05 - 2.77)和1.51(1.02 - 2.22)。
移植肾失功时患有糖尿病的患者存在显著的生存劣势,额外的死亡风险归因于感染和停止透析。