Adkoli Anusha, Smith Colton, Kennedy Timothy, Aikins James, Girda Eugenia
Obstetrics and Gynecology, Rutgers Robert Wood Johnson Medical School, New Brunswick, USA.
Pathology and Laboratory Medicine, Rutgers Robert Wood Johnson Medical School, New Brunswick, USA.
Cureus. 2024 Feb 12;16(2):e54080. doi: 10.7759/cureus.54080. eCollection 2024 Feb.
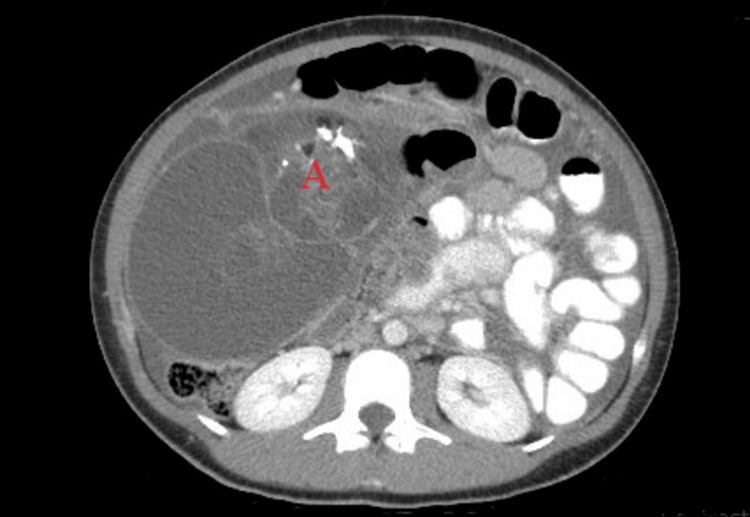
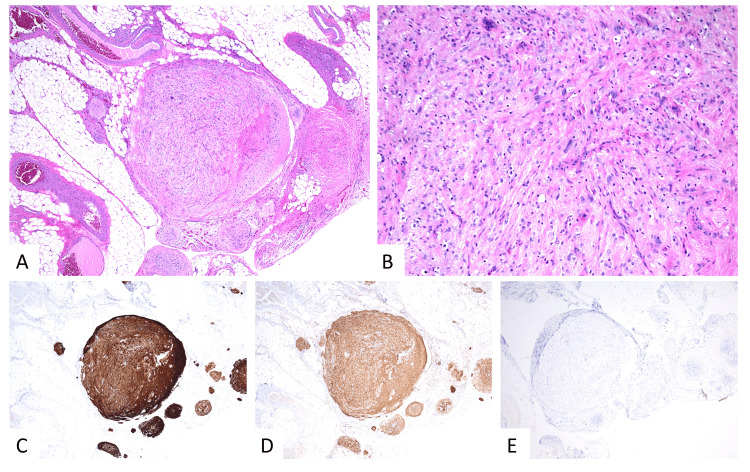
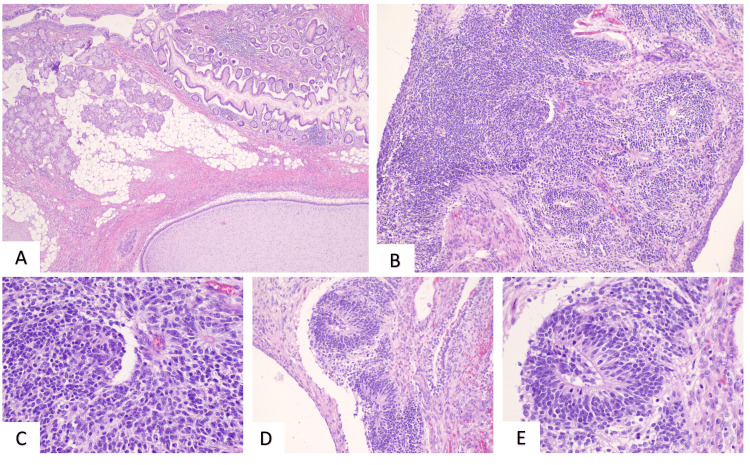
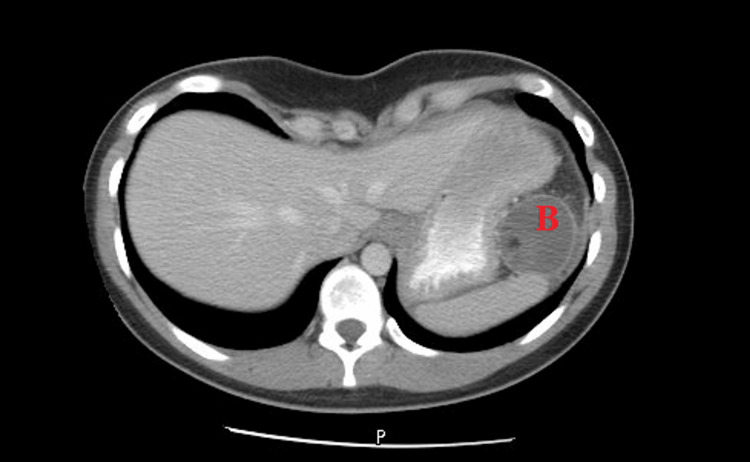
Gliomatosis peritonei (GP) is a rare condition of mature glial tissue within the peritoneum often associated with immature teratomas. This was a case of rapid progression of immature teratoma with splenic lesions and associated GP. The patient was a 21-year-old female who presented with abdominal pain and CT imaging showing suspected malignant teratoma. The patient underwent exploratory laparotomy with fertility-sparing debulking surgery and was diagnosed with stage IIIC grade 3 immature teratoma. She then received adjuvant chemotherapy with bleomycin, etoposide, and cisplatin. Surveillance imaging demonstrated a non-avid splenic lesion. The tumor markers remained normal. She underwent robotic splenectomy and partial peritonectomy with intra-operative findings revealing numerous peritoneal nodules. Follow-up surveillance imaging showed no further lesions. The final histopathology examination demonstrated mature and mesenchymal neural tissue consistent with residual teratoma and no immature elements. The specimens were largely composed of nodules of mature glial tissue and focal areas of mature neuronal tissue. Immunohistochemistry demonstrated glial fibrillary acidic protein (GFAP) and S100 expression, confirming neural origin tissue. Octamer-binding transcription factor 4 (OCT-4) immunostain was negative which confirmed the absence of immature neural tissue. We report a rare case of rapid progression of immature teratoma with splenic metastasis and peritoneal nodules found ultimately to be mature teratoma and associated GP. Recognition of rapidly growing teratoma with new lesions as potential GP is imperative to prevent misdiagnosis as recurrence or progression of disease. This case was treated with secondary debulking surgery which should be a consideration of management if surgically feasible.
腹膜胶质细胞瘤(GP)是一种罕见的腹膜内成熟神经胶质组织疾病,常与未成熟畸胎瘤相关。这是一例未成熟畸胎瘤伴脾脏病变及相关GP快速进展的病例。患者为一名21岁女性,因腹痛就诊,CT成像显示疑似恶性畸胎瘤。患者接受了保留生育功能的减瘤性剖腹探查手术,被诊断为IIIC期3级未成熟畸胎瘤。随后她接受了博来霉素、依托泊苷和顺铂的辅助化疗。监测成像显示脾脏有一个无摄取的病变。肿瘤标志物保持正常。她接受了机器人脾脏切除术和部分腹膜切除术,术中发现有大量腹膜结节。随访监测成像未显示进一步病变。最终的组织病理学检查显示成熟的间充质神经组织,符合残留畸胎瘤,无未成熟成分。标本主要由成熟神经胶质组织结节和成熟神经元组织的局灶区域组成。免疫组化显示胶质纤维酸性蛋白(GFAP)和S100表达,证实为神经源性组织。八聚体结合转录因子4(OCT-4)免疫染色为阴性,证实无未成熟神经组织。我们报告了一例罕见的未成熟畸胎瘤快速进展病例,伴有脾脏转移和腹膜结节,最终发现为成熟畸胎瘤及相关GP。认识到快速生长的畸胎瘤伴新病变可能为潜在的GP对于防止误诊为疾病复发或进展至关重要。该病例接受了二次减瘤手术,如果手术可行,这应作为治疗方案的考虑。