Department of Neurosurgery, Oxford University Hospitals NHS Foundation Trust, Oxford, UK.
Nuffield Department of Surgery, University of Oxford, Oxford, UK.
Acta Neurochir (Wien). 2024 Mar 15;166(1):138. doi: 10.1007/s00701-024-06025-x.
The role of repeat resection for recurrent glioblastoma (rGB) remains equivocal. This study aims to assess the overall survival and complications rates of single or repeat resection for rGB.
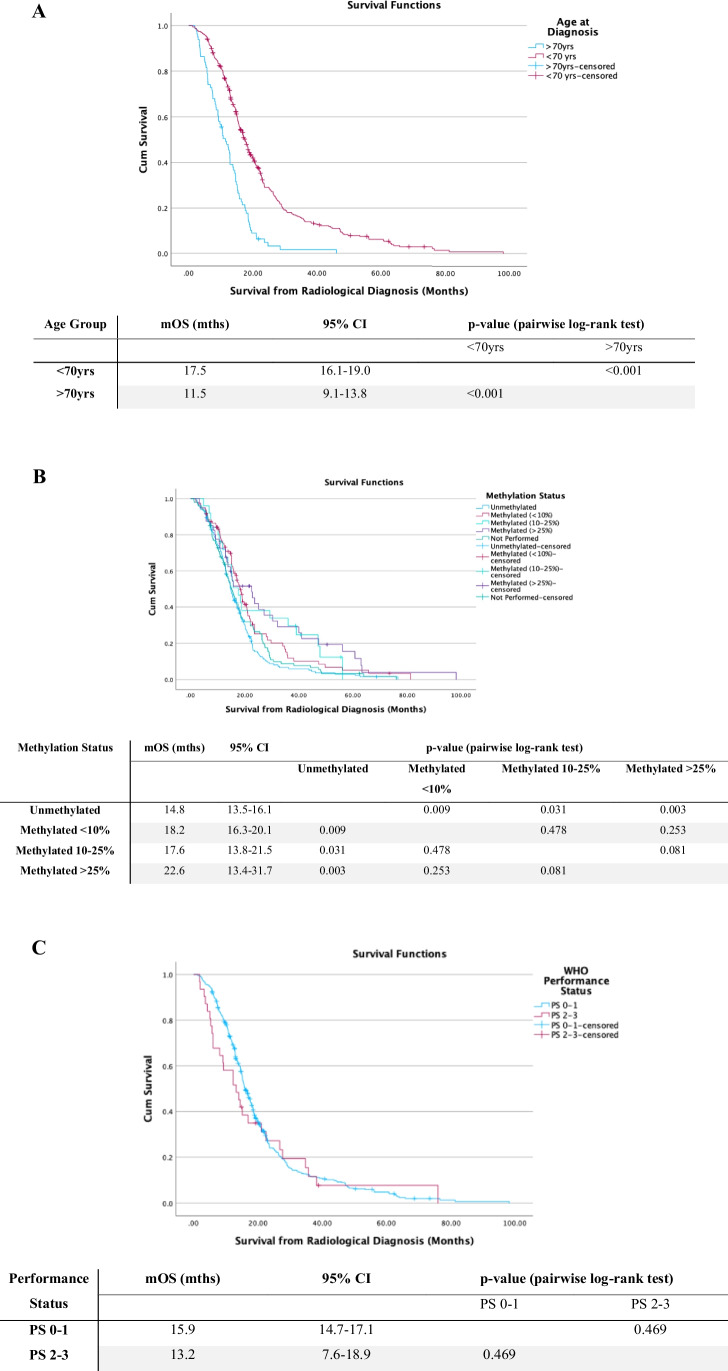
A single-centre retrospective review of all patients with IDH-wildtype glioblastoma managed surgically, between January 2014 and January 2022, was carried out. Patient survival and factors influencing prognosis were analysed, using Kaplan-Meier and Cox regression methods.
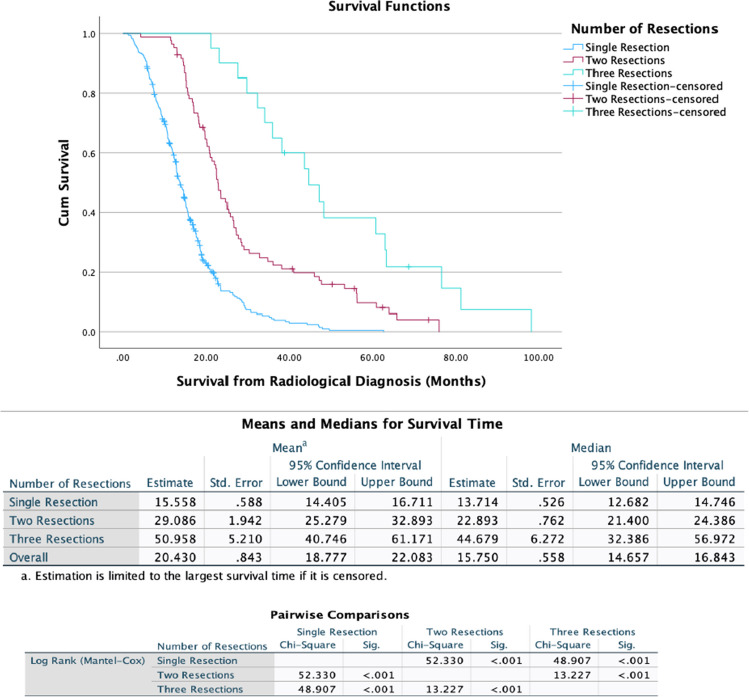
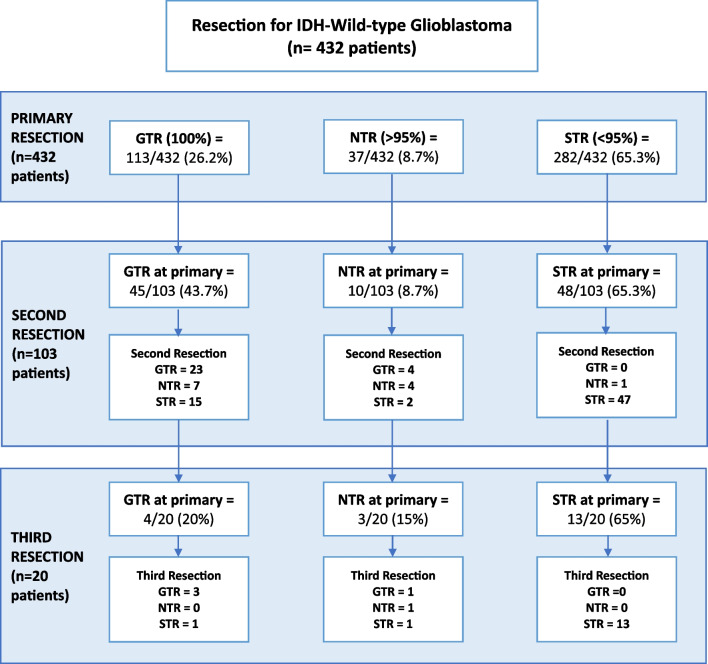
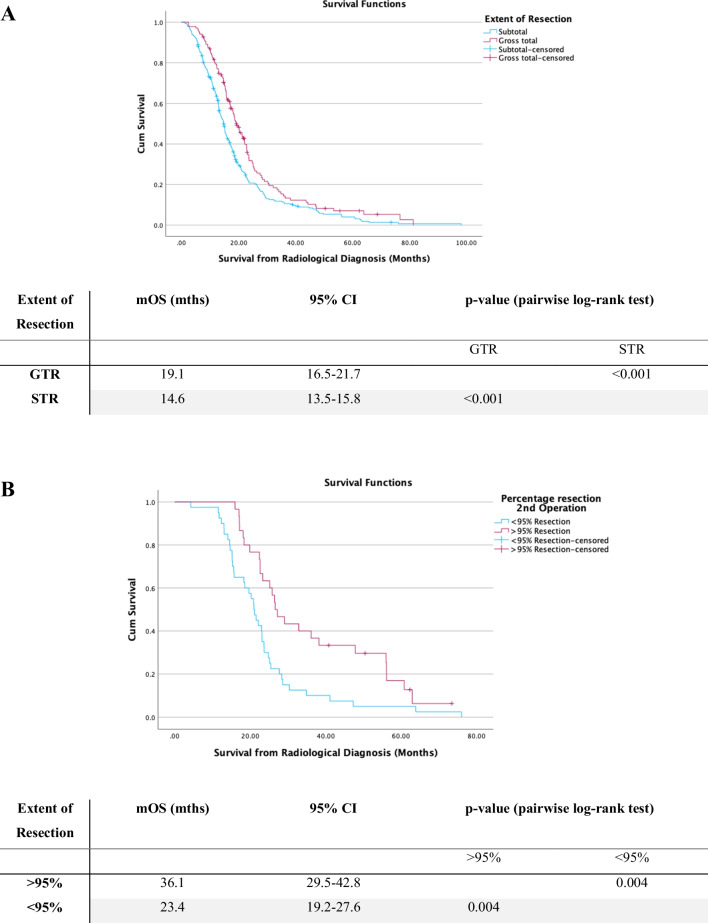
Four hundred thirty-two patients were included, of whom 329 underwent single resection, 83 had two resections and 20 patients underwent three resections. Median OS (mOS) in the cohort who underwent a single operation was 13.7 months (95% CI: 12.7-14.7 months). The mOS was observed to be extended in patients who underwent second or third-time resection, at 22.9 months and 44.7 months respectively (p < 0.001). On second operation achieving > 95% resection or residual tumour volume of < 2.25 cc was significantly associated with prolonged survival. There was no significant difference in overall complication rates between primary versus second (p = 0.973) or third-time resections (p = 0.312). The use of diffusion tensor imaging (DTI) guided resection was associated with reduced post-operative neurological deficit (RR 0.37, p = 0.002), as was use of intraoperative ultrasound (iUSS) (RR 0.45, p = 0.04).
This study demonstrates potential prolongation of survival for rGB patients undergoing repeat resection, without significant increase in complication rates with repeat resections. Achieving a more complete repeat resection improved survival. Moreover, the use of intraoperative imaging adjuncts can maximise tumour resection, whilst minimising the risk of neurological deficit.
复发性胶质母细胞瘤(rGB)再次切除的作用仍存在争议。本研究旨在评估单发性或复发性 rGB 切除的总生存率和并发症发生率。
对 2014 年 1 月至 2022 年 1 月期间在单中心接受手术治疗的 IDH 野生型胶质母细胞瘤患者进行回顾性分析。采用 Kaplan-Meier 和 Cox 回归方法分析患者的生存情况和影响预后的因素。
共纳入 432 例患者,其中 329 例行单发性切除术,83 例行二次切除术,20 例行三次切除术。单发性手术组的中位总生存期(mOS)为 13.7 个月(95%CI:12.7-14.7 个月)。二次或三次手术的 mOS 分别延长至 22.9 个月和 44.7 个月(p<0.001)。第二次手术达到>95%切除或残余肿瘤体积<2.25cc 与延长生存时间显著相关。原发性与二次(p=0.973)或三次(p=0.312)手术的总体并发症发生率无显著差异。弥散张量成像(DTI)引导切除与术后神经功能缺损减少相关(RR 0.37,p=0.002),术中超声(iUSS)也与术后神经功能缺损减少相关(RR 0.45,p=0.04)。
本研究表明,rGB 患者再次切除可能延长生存时间,而多次切除并不会显著增加并发症发生率。实现更完全的重复切除可改善生存。此外,术中使用影像学辅助手段可以最大限度地切除肿瘤,同时最大限度地降低神经功能缺损的风险。