Saporito Gennaro, Gentili Luca, Cacchio Angelo, Casalena Alfonsina, Necozione Stefano, Ricci Alessandro, Venturoni Federica, Marinangeli Franco, Pistoia Francesca
Department of Biotechnological and Applied Clinical Sciences, Intensive Care, and Pain Treatment, University of L'Aquila, L'Aquila, Italy.
Department of Anesthesia and Intensive Care Unit, Mazzini Hospital, Teramo, Italy.
Neurotrauma Rep. 2024 Mar 14;5(1):267-276. doi: 10.1089/neur.2023.0120. eCollection 2024.
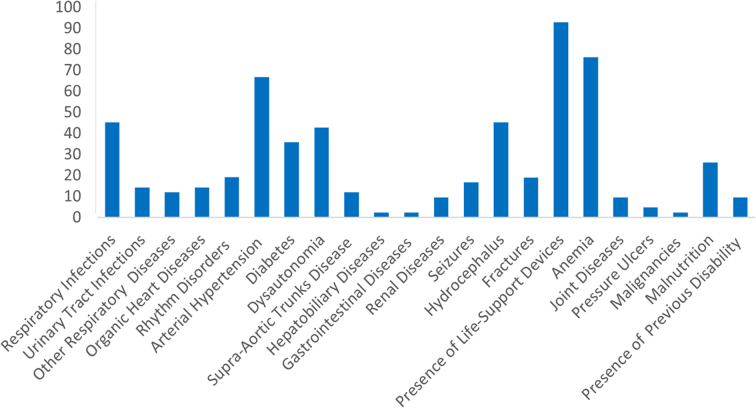
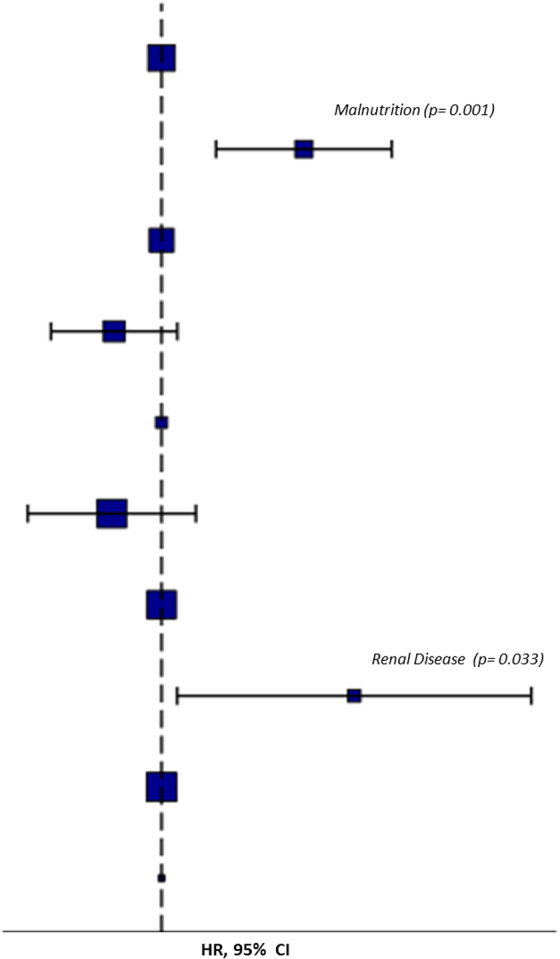
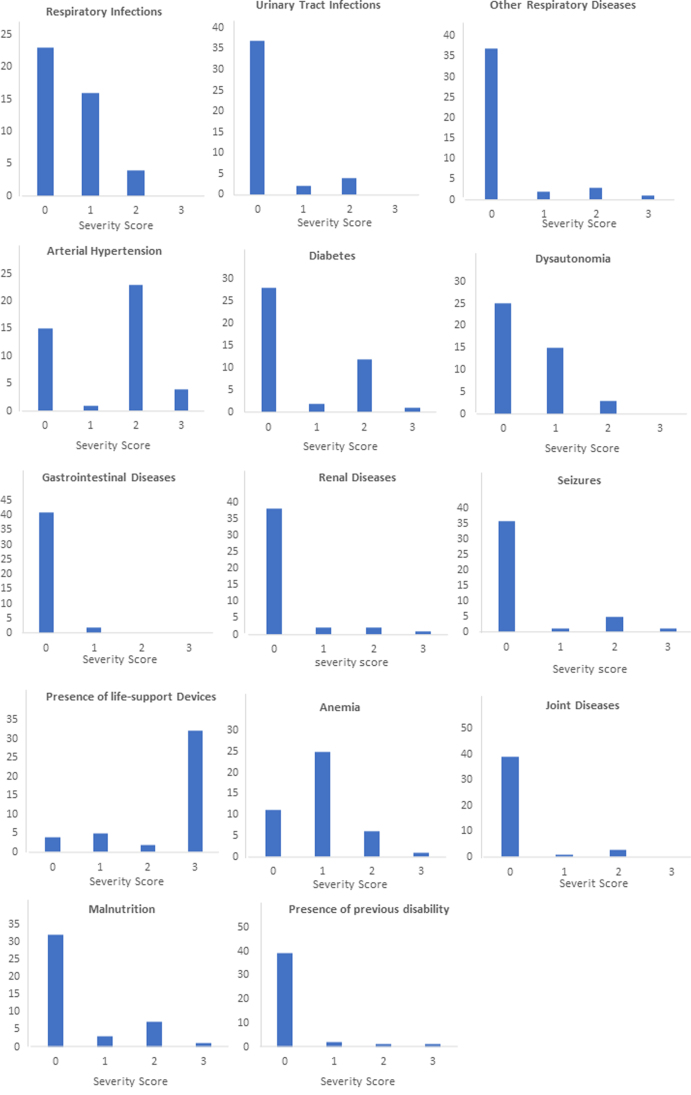
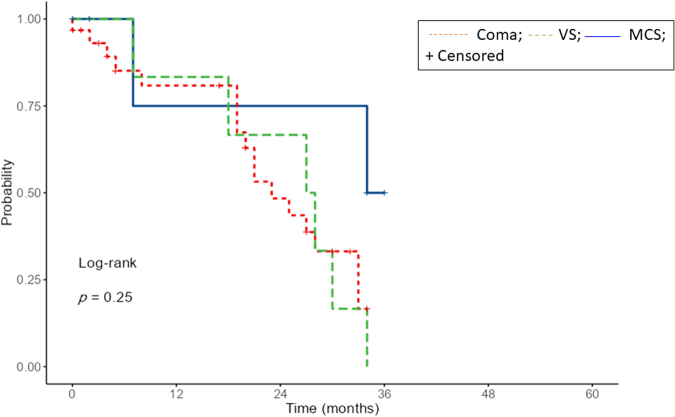
Medical comorbidities are frequent in patients with disorders of consciousness (DoC) and their impact on outcomes is under investigation. The aim of this study was to investigate patients with DoC in the acute stage and the influence of comorbidities. Patients admitted to intensive care units and neurological units with a diagnosis of coma, vegetative state/unresponsive wakefulness syndrome (VS/UWS), and minimally conscious state (MCS) were investigated through the Glasgow Coma Scale (GCS), the Coma Recovery Scale - Revised (CRS-R) and the Comorbidities Coma Scale (CoCos). Forty-three patients (21 men and 22 women; mean age at admission: 60.4 ± 21.0) were included in the study. The most frequent diagnosis at admission was coma (72%) followed by VS/UWS (14%) and MCS (14%). The most frequent brain injury was subarachnoid hemorrhage (46%). At the 6-month follow-up, 19 patients had died (44%), 15 showed a full recovery of consciousness (35%), 7 were in a condition of emergence from MCS (16%), and 2 showed a persistent VS/UWS (5%). Forty-two (98%) patients showed at least one comorbidity: presence of life-support device (92.9%), anemia (76.2%), arterial hypertension (66,7%), hydrocephalus (45.3%), and respiratory infections (45.2%) were those most frequently reported. At the Multivariable Cox regression, the presence of renal disease (hazard ratio [HR] 33.37; = 0.033) and malnutrition (HR 14.52; = 0.001) were predictors of missed recovery of full consciousness. Although adverse outcomes are generally predicted by the severity of brain damage, the presence of medical comorbidities in an acute phase could influence outcomes and long-term prognosis.
意识障碍(DoC)患者常伴有多种医学合并症,其对预后的影响正在研究中。本研究旨在调查急性期意识障碍患者及其合并症的影响。通过格拉斯哥昏迷量表(GCS)、修订版昏迷恢复量表(CRS-R)和合并症昏迷量表(CoCos)对入住重症监护病房和神经科病房、诊断为昏迷、植物状态/无反应觉醒综合征(VS/UWS)和最低意识状态(MCS)的患者进行调查。本研究纳入了43例患者(21例男性和22例女性;入院时平均年龄:60.4±21.0)。入院时最常见的诊断是昏迷(72%),其次是VS/UWS(14%)和MCS(14%)。最常见的脑损伤是蛛网膜下腔出血(46%)。在6个月的随访中,19例患者死亡(44%),15例意识完全恢复(35%),7例从MCS状态中苏醒(16%),2例持续处于VS/UWS状态(5%)。42例(98%)患者至少有一种合并症:最常报告的是存在生命支持设备(92.9%)、贫血(76.2%)、动脉高血压(66.7%)、脑积水(45.3%)和呼吸道感染(45.2%)。在多变量Cox回归分析中,肾病(风险比[HR]33.37;P=0.033)和营养不良(HR 14.52;P=0.001)是意识未能完全恢复的预测因素。虽然不良预后通常由脑损伤的严重程度预测,但急性期医学合并症的存在可能会影响预后和长期预后。