From the Diagnostic and Interventional Radiology, University Hospital Zurich, University of Zurich, Zurich, Switzerland (T.S., L.J.M., H.A.); Department of Radiology and Nuclear Medicine, Maastricht University Medical Center, Maastricht, the Netherlands (T.S., M.C.M., L.S., B.M., T.G.F., J.E.W.); CARIM School for Cardiovascular Diseases, Maastricht University, Maastricht, the Netherlands (T.S., M.C.M., L.S., B.M., J.E.W.); Bayer AG, Berlin, Germany (M.C.M., G.J., H.P.); and Computed Tomography Division, Siemens Healthineers AG (R.G., T.N., B.S., T.G.F.), Forchheim, Germany.
Invest Radiol. 2024 Oct 1;59(10):677-683. doi: 10.1097/RLI.0000000000001073. Epub 2024 Mar 25.
Calcified plaques induce blooming artifacts in coronary computed tomography angiography (CCTA) potentially leading to inaccurate stenosis evaluation. Tungsten represents a high atomic number, experimental contrast agent with different physical properties than iodine. We explored the potential of a tungsten-based contrast agent for photon-counting detector (PCD) CCTA in heavily calcified coronary vessels.
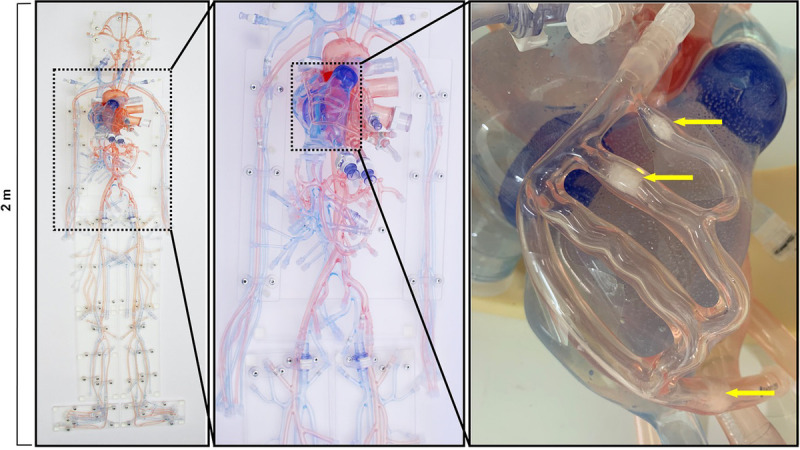
A cardiovascular phantom exhibiting coronaries with calcified plaques was imaged on a first-generation dual-source PCD-CT. The coronaries with 3 different calcified plaques were filled with iodine and tungsten contrast media solutions equating to iodine and tungsten delivery rates (IDR and TDR) of 0.3, 0.5, 0.7, 1.0, 1.5, 2.0, 2.5, and 3.0 g/s, respectively. Electrocardiogram-triggered sequential acquisitions were performed in the spectral mode (QuantumPlus). Virtual monoenergetic images (VMIs) were reconstructed from 40 to 190 keV in 1 keV increments. Blooming artifacts and percentage error stenoses from calcified plaques were quantified, and attenuation characteristics of both contrast media were recorded.
Blooming artifacts from calcified plaques were most pronounced at 40 keV (78%) and least pronounced at 190 keV (58%). Similarly, percentage error stenoses were highest at 40 keV (48%) and lowest at 190 keV (2%), respectively. Attenuation of iodine decreased monotonically in VMIs from low to high keV, with the strongest decrease from 40 keV to 100 keV (IDR of 2.5 g/s: 1279 HU at 40 keV, 187 HU at 100 kV, and 35 HU at 190 keV). The attenuation of tungsten, on the other hand, increased monotonically as a function of VMI energy, with the strongest increase between 40 and 100 keV (TDR of 2.5 g/s: 202 HU at 40 keV, 661 HU at 100 kV, and 717 HU at 190 keV). For each keV level, the relationship between attenuation and IDR/TDR could be described by linear regressions ( R2 ≥ 0.88, P < 0.001). Specifically, attenuation increased linearly when increasing the delivery rate irrespective of keV level or contrast medium. Iodine exhibited the highest relative increase in attenuation values at lower keV levels when increasing the IDR. Conversely, for tungsten, the greatest relative increase in attenuation values occurred at higher keV levels when increasing the TDR. When high keV imaging is desirable to reduce blooming artifacts from calcified plaques, IDR has to be increased at higher keV levels to maintain diagnostic vessel attenuation (ie, 300 HU), whereas for tungsten, TDR can be kept constant or can be even reduced at high keV energy levels.
Tungsten's attenuation characteristics in relation to VMI energy levels are reversed to those of iodine, with tungsten exhibiting high attenuation values at high keV levels and vice versa. Thus, tungsten shows promise for high keV imaging CCTA with PCD-CT as-in distinction to iodine-both high vessel attenuation and low blooming artifacts from calcified plaques can be achieved.
钙化斑块在冠状动脉计算机断层血管造影(CCTA)中会产生“blooming”伪影,可能导致狭窄程度评估不准确。钨是一种具有高原子序数的实验性对比剂,其物理性质与碘不同。我们探索了基于钨的对比剂在重度钙化冠状动脉中的应用潜力。
使用具有钙化斑块的冠状动脉的心血管体模,在第一代双源光子计数探测器(PCD)CT 上进行成像。使用碘和钨对比剂溶液填充 3 种不同钙化斑块的冠状动脉,其碘和钨输送率(IDR 和 TDR)分别为 0.3、0.5、0.7、1.0、1.5、2.0、2.5 和 3.0 g/s。使用心电图触发的顺序采集在光谱模式(QuantumPlus)下进行。从 40 到 190 keV 以 1 keV 的增量重建虚拟单能量图像(VMIs)。量化钙化斑块的blooming 伪影和百分比误差狭窄,并记录两种对比剂的衰减特性。
钙化斑块的 blooming 伪影在 40 keV 时最为明显(78%),在 190 keV 时最为不明显(58%)。同样,百分比误差狭窄在 40 keV 时最高(48%),在 190 keV 时最低(2%)。碘的衰减在 VMIs 中从低能到高能单调下降,从 40 keV 到 100 keV 下降最强(IDR 为 2.5 g/s:40 keV 时 1279 HU,100 keV 时 187 HU,190 keV 时 35 HU)。另一方面,钨的衰减随着 VMI 能量的增加而单调增加,在 40 到 100 keV 之间增加最强(TDR 为 2.5 g/s:40 keV 时 202 HU,100 keV 时 661 HU,190 keV 时 717 HU)。对于每个 keV 水平,衰减与 IDR/TDR 之间的关系都可以用线性回归来描述(R2≥0.88,P<0.001)。具体来说,无论 keV 水平或对比剂如何,增加输送率都会导致衰减线性增加。当增加 IDR 时,碘在较低 keV 水平下的衰减值具有较高的相对增加。相反,对于钨,当增加 TDR 时,衰减值的相对增加最大发生在较高的 keV 水平。当需要高 keV 成像以减少钙化斑块的 blooming 伪影时,必须在较高的 keV 水平上增加 IDR,以维持诊断性血管衰减(即 300 HU),而对于钨,TDR 可以保持不变,甚至可以在高 keV 能量水平上降低。
钨的衰减特性与 VMIs 能级的关系与碘相反,钨在高能级时表现出高衰减值,反之亦然。因此,钨有望用于 PCD-CT 的高 keV 成像 CCTA,与碘不同,它既能实现高血管衰减,又能降低钙化斑块的 blooming 伪影。