Hesse Kerrick
Sunderland Royal Hospital, Kayll Road, Sunderland SR4 7TP, UK.
Am Heart J Plus. 2022 Oct 17;23:100218. doi: 10.1016/j.ahjo.2022.100218. eCollection 2022 Nov.
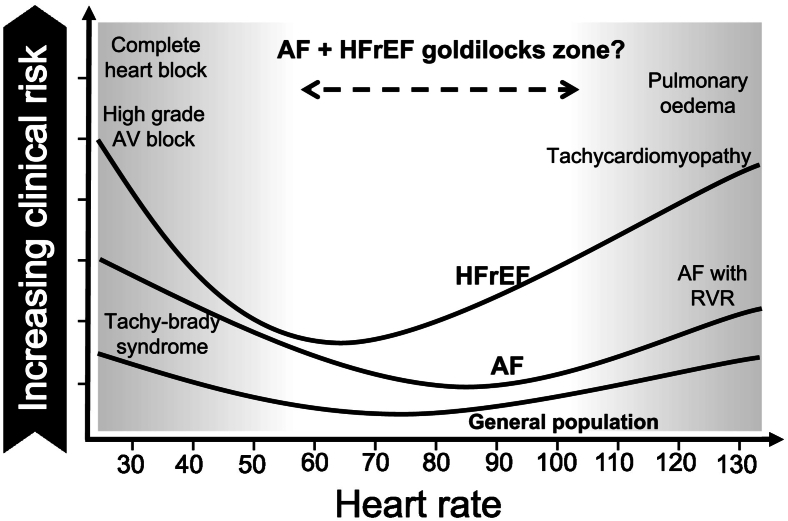
The rates of atrial fibrillation (AF) and heart failure with reduced ejection fraction (HFrEF) continue to grow with many patients suffering from their combined impact on quality of life and prognosis. A lower heart rate (HR) in HFrEF is associated with reduced morbidity and mortality due to beta-blocker and ivabradine therapy. Postulated mechanisms include reduced neurohumoral activation, increased diastolic filling time and myocardial energy conservation. In contrast, the landmark randomised controlled non-inferiority RACE II trial demonstrated that a lenient rate control strategy (target HR <110 beats per minute [bpm]) was more attainable and safer than a strict rate control strategy (resting HR <80 bpm) in permanent AF. Physiologically, a higher HR is needed to compensate for the lost 'atrial kick' that contributes to the cardiac output by coordinated atrial contractions in normal sinus rhythm. This leaves the not insignificant number of patients with HFrEF and AF in a conundrum over optimal HR control. Retrospective analyses of AF and HR control in landmark HFrEF trials (e.g. CHARM, PARADIGM and ATMOSPHERE) point towards better outcomes with a less stringent target HR. However, this association disappears after adjustment for known prognostic markers in HFrEF, including left ventricular ejection fraction, New York Heart Association class and NT-proBNP levels. There is a clear need for dedicated randomised controlled trials, investigating rate control strategies in this increasingly large subgroup of patients. Regardless of rate control strategy, effective anti-coagulation and guideline-directed medical therapy must not be forgotten in the treatment of patients with HFrEF and AF.
心房颤动(AF)和射血分数降低的心力衰竭(HFrEF)的发病率持续上升,许多患者深受其对生活质量和预后的综合影响。HFrEF患者心率降低与β受体阻滞剂和伊伐布雷定治疗导致的发病率和死亡率降低相关。推测的机制包括减少神经体液激活、增加舒张期充盈时间和心肌能量保存。相比之下,具有里程碑意义的随机对照非劣效性RACE II试验表明,在永久性房颤中,宽松心率控制策略(目标心率<110次/分钟[bpm])比严格心率控制策略(静息心率<80 bpm)更易于实现且更安全。从生理角度来看,需要更高的心率来补偿正常窦性心律时心房协调收缩对心输出量有贡献的“心房辅助泵”丧失。这使得相当数量的HFrEF合并AF患者在最佳心率控制方面陷入困境。对具有里程碑意义的HFrEF试验(如CHARM、PARADIGM和ATMOSPHERE)中AF和心率控制的回顾性分析表明,目标心率不太严格时预后更好。然而,在对HFrEF中已知的预后标志物(包括左心室射血分数、纽约心脏协会分级和NT-proBNP水平)进行调整后,这种关联消失。显然需要专门的随机对照试验来研究这一不断扩大的患者亚组中的心率控制策略。无论心率控制策略如何,在治疗HFrEF合并AF患者时,都不能忘记有效的抗凝和指南指导的药物治疗。