Cellular and Molecular Cardiology Lab IRCCS L. Spallanzani Rome Italy.
Department of Clinical, Internal, Anesthesiology and Cardiovascular Sciences Sapienza University of Rome Rome Italy.
J Am Heart Assoc. 2024 Apr 16;13(8):e032734. doi: 10.1161/JAHA.123.032734. Epub 2024 Apr 2.
The limited ability of enzyme replacement therapy (ERT) in removing globotriaosylceramide from cardiomyocytes is recognized for advanced Fabry disease cardiomyopathy (FDCM). Prehypertrophic FDCM is believed to be cured or stabilized by ERT. However, no pathologic confirmation is available. We report here on the long-term clinical-pathologic impact of ERT on prehypertrophic FDCM.
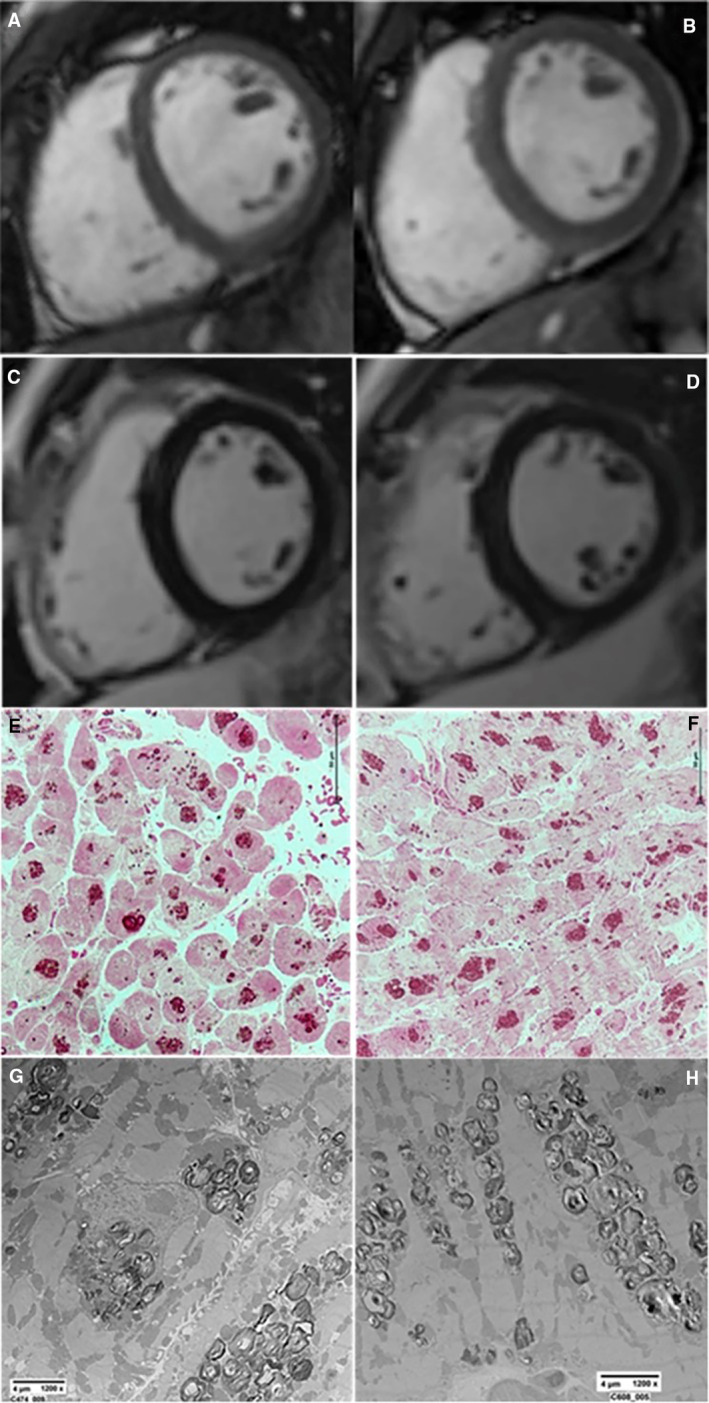
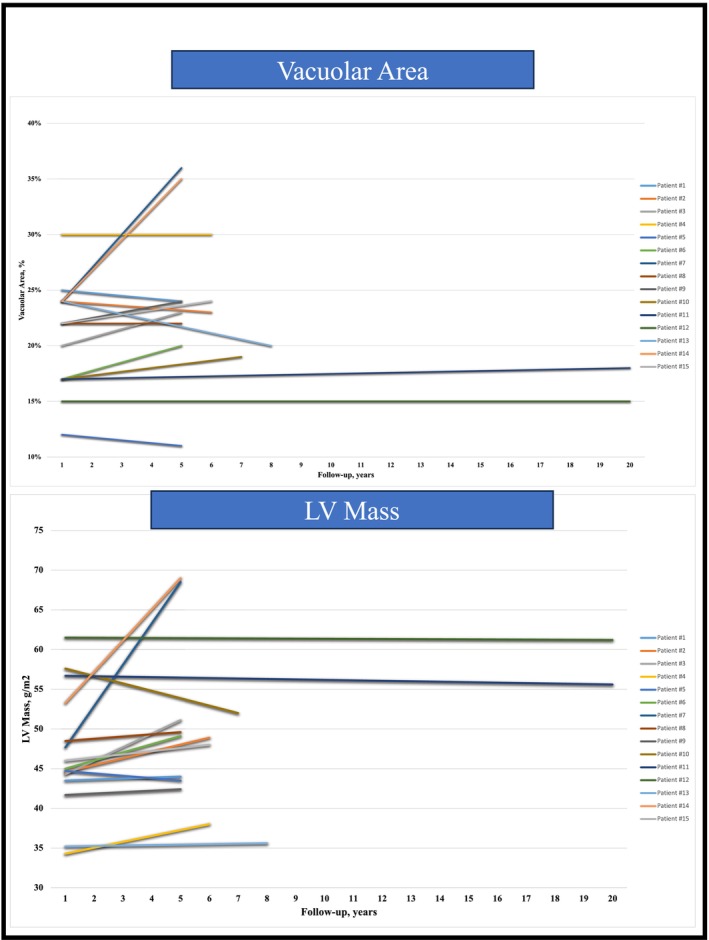
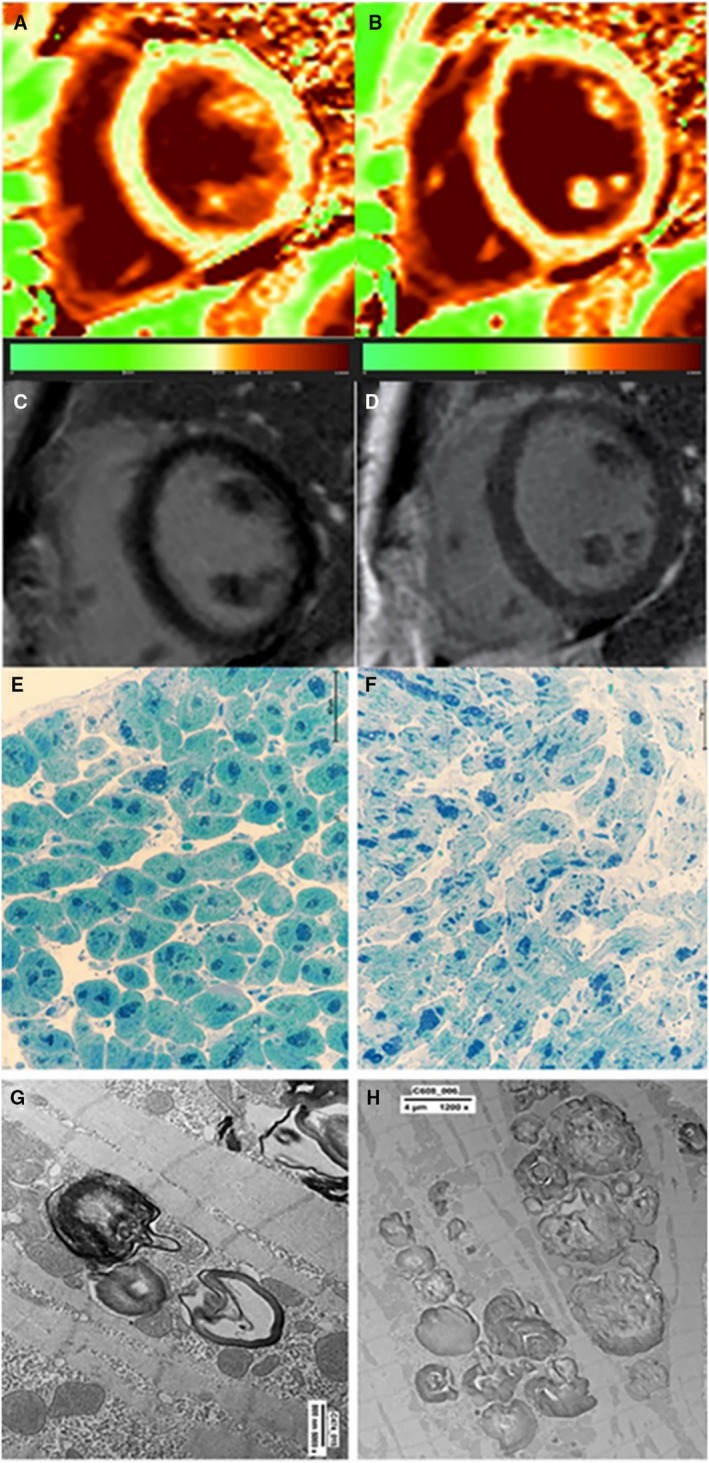
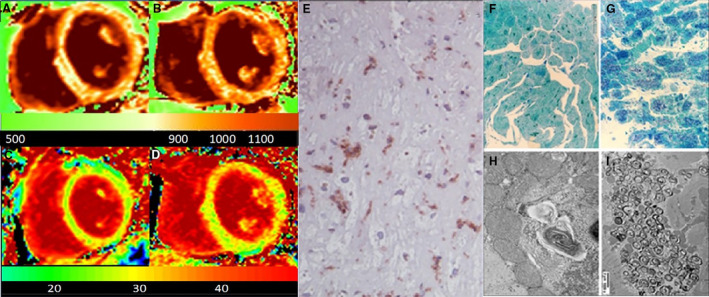
Fifteen patients with Fabry disease with left ventricular maximal wall thickness ≤10.5 mm at cardiac magnetic resonance required endomyocardial biopsy because of angina and ventricular arrhythmias. Endomyocardial biopsy showed coronary small-vessel disease in the angina cohort, and vacuoles in smooth muscle cells and cardiomyocytes ≈20% of the cell surface containing myelin bodies at electron microscopy. Patients received α-agalsidase in 8 cases, and β-agalsidase in 7 cases. Both groups experienced symptom improvement except 1 patients treated with α-agalsidase and 1 treated with β-agalsidase. After ERT administration ranging from 4 to 20 years, all patients had control cardiac magnetic resonance and left ventricular endomyocardial biopsy because of persistence of symptoms or patient inquiry on disease resolution. In 13 asymptomatic patients with FDCM, left ventricular maximal wall thickness and left ventricular mass, cardiomyocyte diameter, vacuole surface/cell surface ratio, and vessels remained unchanged or minimally increased (left ventricular mass increased by <2%) even after 20 years of observation, and storage material was still present at electron microscopy. In 2 symptomatic patients, FDCM progressed, with larger and more engulfed by globotriaosylceramide myocytes being associated with myocardial virus-negative lymphocytic inflammation.
ERT stabilizes storage deposits and myocyte dimensions in 87% of patients with prehypertrophic FDCM. Globotriaosylceramide is never completely removed even after long-term treatment. Immune-mediated myocardial inflammation can overlap, limiting ERT activity.
酶替代疗法(ERT)去除心肌细胞中的神经酰胺三己糖苷的能力有限,这已被公认是晚期法布里病心肌病(FDCM)的原因。人们认为,肥厚前期 FDCM 可以通过 ERT 治愈或稳定。然而,目前尚无病理确认。我们在此报告 ERT 对肥厚前期 FDCM 的长期临床病理影响。
15 名 Fabry 病患者因心绞痛和室性心律失常需要进行心内膜心肌活检,其左心室最大壁厚度≤10.5mm。心内膜心肌活检显示心绞痛组存在冠状动脉小血管疾病,电镜下平滑肌细胞和心肌细胞中约 20%的细胞膜表面有空泡,其中含有髓鞘体。8 例患者接受α-半乳糖苷酶治疗,7 例患者接受β-半乳糖苷酶治疗。除 1 例接受α-半乳糖苷酶治疗和 1 例接受β-半乳糖苷酶治疗的患者外,两组患者均出现症状改善。ERT 治疗后 4 至 20 年,所有患者均因症状持续或患者询问疾病是否痊愈而进行了心脏磁共振和左心室心内膜心肌活检控制。在 13 例无症状 FDCM 患者中,左心室最大壁厚度和左心室质量、心肌细胞直径、空泡面积/细胞面积比以及血管均无变化或仅轻度增加(左心室质量增加<2%),即使经过 20 年的观察,电镜下仍存在贮存物质。在 2 例有症状的患者中,FDCM 进展,有更多的肌细胞被神经酰胺三己糖苷吞噬,且伴有心肌病毒阴性的淋巴细胞炎症。
ERT 稳定了 87%肥厚前期 FDCM 患者的贮存物沉积和心肌细胞尺寸。即使经过长期治疗,神经酰胺三己糖苷也从未完全清除。免疫介导的心肌炎症可能会重叠,限制 ERT 的活性。